

Patient and Institutional Characteristics Influence the Decision to Use Extracorporeal Cardiopulmonary Resuscitation for In-Hospital Cardiac Arrest
- PMID: 32347147
- PMCID: PMC7428578
- DOI: 10.1161/JAHA.119.015522
Patient and Institutional Characteristics Influence the Decision to Use Extracorporeal Cardiopulmonary Resuscitation for In-Hospital Cardiac Arrest
Abstract
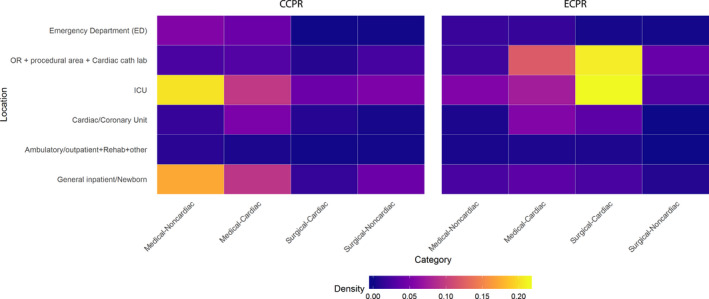
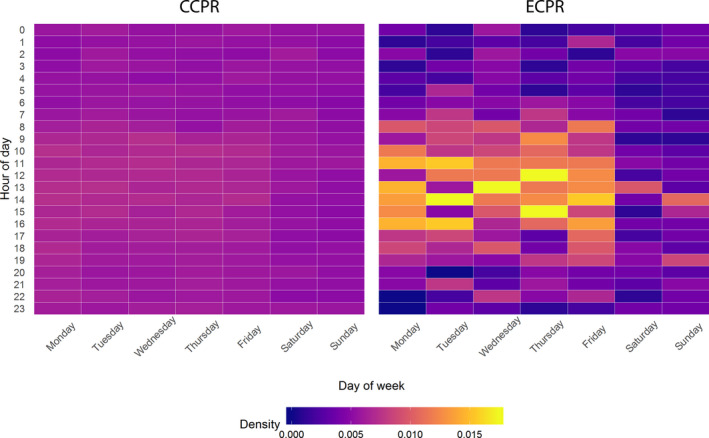
BACKGROUND Outcomes from extracorporeal cardiopulmonary resuscitation (ECPR) are felt to be influenced by selective use, but the characteristics of those receiving ECPR are undefined. We demonstrate the relationship between individual patient and hospital characteristics and the probability of ECPR use. METHODS AND RESULTS We performed an observational analysis of adult inpatient cardiac arrests in the United States from 2000 to 2018 reported to the American Heart Association's Get With The Guidelines-Resuscitation registry restricted to hospitals that provided ECPR. We calculated case mix adjusted relative risk (RR) of receiving ECPR for individual characteristics. From 2000 to 2018, 129 736 patients had a cardiac arrest (128 654 conventional cardiopulmonary resuscitation and 1082 ECPR) in 224 hospitals that offered ECPR. ECPR use was associated with younger age (RR, 1.5 for <40 vs. 40-59 years; 95% CI, 1.2-1.8), no pre-existing comorbidities (RR, 1.4; 95% CI, 1.1-1.8) or cardiac-specific comorbidities (congestive heart failure [RR, 1.3; 95% CI, 1.2-1.5], prior myocardial infarction [RR, 1.4; 95% CI, 1.2-1.6], or current myocardial infarction [RR, 1.5; 95% CI, 1.3-1.8]), and in locations of procedural areas at the times of cardiac arrest (RR, 12.0; 95% CI, 9.5-15.1). ECPR decreased after hours (3-11 pm [RR, 0.8; 95% CI, 0.7-1.0] and 11 pm-7 am [RR, 0.6; 95% CI, 0.5-0.7]) and on weekends (RR, 0.7; 95% CI, 0.6-0.9). CONCLUSIONS Less than 1% of in-hospital cardiac arrest patients are treated with ECPR. ECPR use is influenced by patient age, comorbidities, and hospital system factors. Randomized controlled trials are needed to better define the patients in whom ECPR may provide a benefit.
Keywords: cardiopulmonary resuscitation; extracorporeal cardiopulmonary resuscitation; extracorporeal life support; extracorporeal membrane oxygenation; in‐hospital cardiac arrest; resuscitation.
Figures
References
-
- Yannopoulos D, Bartos JA, Martin C, Raveendran G, Missov E, Conterato M, Frascone RJ, Trembley A, Sipprell K, John R, et al. Minnesota Resuscitation Consortium's advanced perfusion and reperfusion cardiac life support strategy for out‐of‐hospital refractory ventricular fibrillation. J Am Heart Assoc. 2016;5:e003732 DOI: 10.1161/JAHA.116.003732. - DOI - PMC - PubMed
-
- Stub D, Bernard S, Pellegrino V, Smith K, Walker T, Sheldrake J, Hockings L, Shaw J, Duffy SJ, Burrell A, et al. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion (the CHEER trial). Resuscitation. 2015;86:88–94. - PubMed
-
- Sakamoto T, Morimura N, Nagao K, Asai Y, Yokota H, Nara S, Hase M, Tahara Y, Atsumi T, SAVE‐J Study Group . Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out‐of‐hospital cardiac arrest: a prospective observational study. Resuscitation. 2014;85:762–768. - PubMed
-
- Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, Chen WJ, Huang SC, Chi NH, Wang CH, et al. Cardiopulmonary resuscitation with assisted extracorporeal life‐support versus conventional cardiopulmonary resuscitation in adults with in‐hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008;372:554–561. - PubMed
-
- Maekawa K, Tanno K, Hase M, Mori K, Asai Y. Extracorporeal cardiopulmonary resuscitation for patients with out‐of‐hospital cardiac arrest of cardiac origin. Crit Care Med. 2013;41:1186–1196. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
