

Deep learning in rare disease. Detection of tubers in tuberous sclerosis complex
- PMID: 32348367
- PMCID: PMC7190137
- DOI: 10.1371/journal.pone.0232376
Deep learning in rare disease. Detection of tubers in tuberous sclerosis complex
Abstract
Objective: To develop and test a deep learning algorithm to automatically detect cortical tubers in magnetic resonance imaging (MRI), to explore the utility of deep learning in rare disorders with limited data, and to generate an open-access deep learning standalone application.
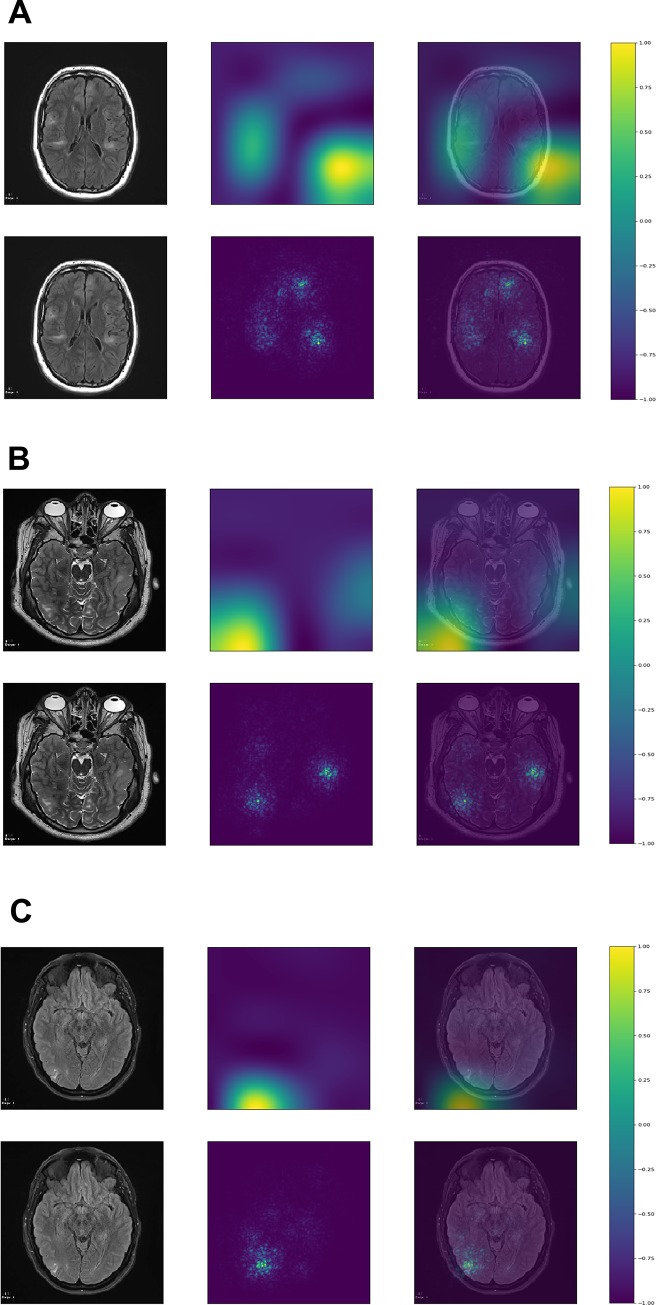
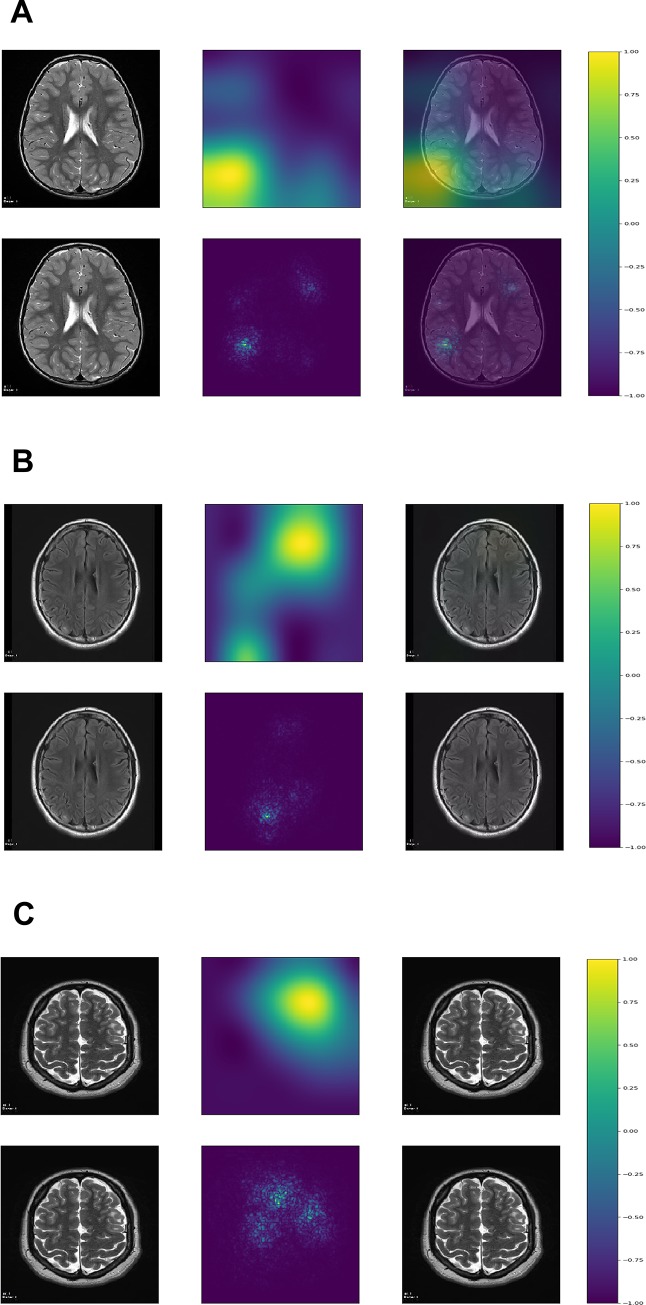
Methods: T2 and FLAIR axial images with and without tubers were extracted from MRIs of patients with tuberous sclerosis complex (TSC) and controls, respectively. We trained three different convolutional neural network (CNN) architectures on a training dataset and selected the one with the lowest binary cross-entropy loss in the validation dataset, which was evaluated on the testing dataset. We visualized image regions most relevant for classification with gradient-weighted class activation maps (Grad-CAM) and saliency maps.
Results: 114 patients with TSC and 114 controls were divided into a training set, a validation set, and a testing set. The InceptionV3 CNN architecture performed best in the validation set and was evaluated in the testing set with the following results: sensitivity: 0.95, specificity: 0.95, positive predictive value: 0.94, negative predictive value: 0.95, F1-score: 0.95, accuracy: 0.95, and area under the curve: 0.99. Grad-CAM and saliency maps showed that tubers resided in regions most relevant for image classification within each image. A stand-alone trained deep learning App was able to classify images using local computers with various operating systems.
Conclusion: This study shows that deep learning algorithms are able to detect tubers in selected MRI images, and deep learning can be prudently applied clinically to manually selected data in a rare neurological disorder.
Conflict of interest statement
ISF has received an Amazon Web Services Cloud Credits for Research support in the form of computational credits for his project on “Identification and localization of tubers in Tuberous Sclerosis Complex with deep learning convolutional neural networks”. JYW, DK, HN, MEB, MS, and JP received funding to collect the data as a part of the TACERN collaborative. There are no patents, products in development or marketed products to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- O'Callaghan FJ, Shiell AW, Osborne JP, Martyn CN. Prevalence of tuberous sclerosis estimated by capture-recapture analysis. Lancet. 1998;351(9114):1490. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
