

Electroencephalogram Burst-suppression during Cardiopulmonary Bypass in Elderly Patients Mediates Postoperative Delirium
- PMID: 32349072
- PMCID: PMC7365754
- DOI: 10.1097/ALN.0000000000003328
Electroencephalogram Burst-suppression during Cardiopulmonary Bypass in Elderly Patients Mediates Postoperative Delirium
Abstract
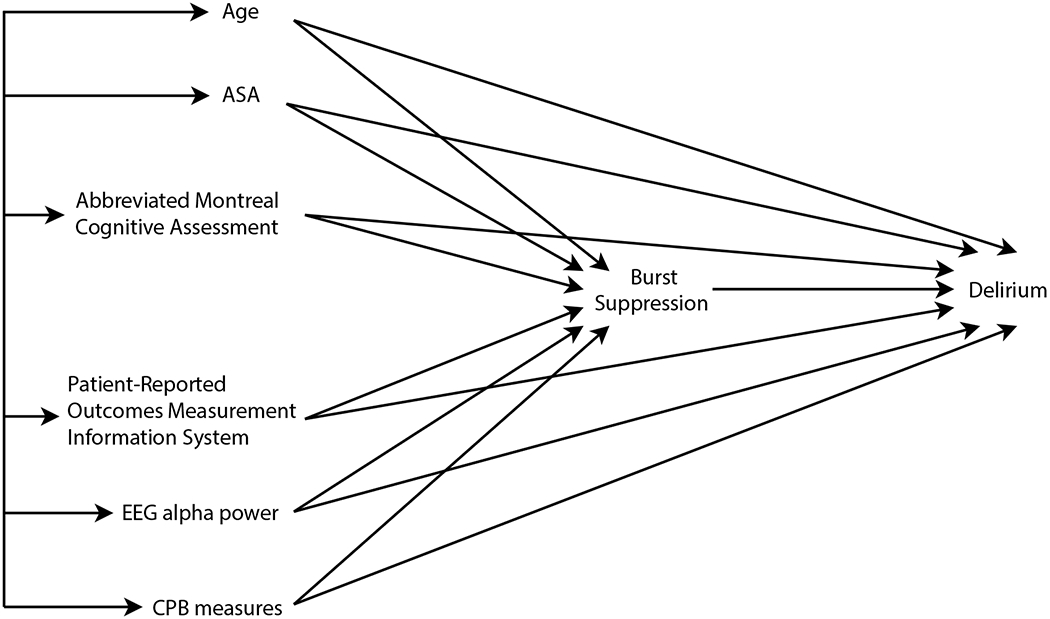
Background: Intraoperative burst-suppression is associated with postoperative delirium. Whether this association is causal remains unclear. Therefore, the authors investigated whether burst-suppression during cardiopulmonary bypass (CPB) mediates the effects of known delirium risk factors on postoperative delirium.
Methods: This was a retrospective cohort observational substudy of the Minimizing ICU [intensive care unit] Neurological Dysfunction with Dexmedetomidine-induced Sleep (MINDDS) trial. The authors analyzed data from patients more than 60 yr old undergoing cardiac surgery (n = 159). Univariate and multivariable regression analyses were performed to assess for associations and enable causal inference. Delirium risk factors were evaluated using the abbreviated Montreal Cognitive Assessment and Patient-Reported Outcomes Measurement Information System questionnaires for applied cognition, physical function, global health, sleep, and pain. The authors also analyzed electroencephalogram data (n = 141).
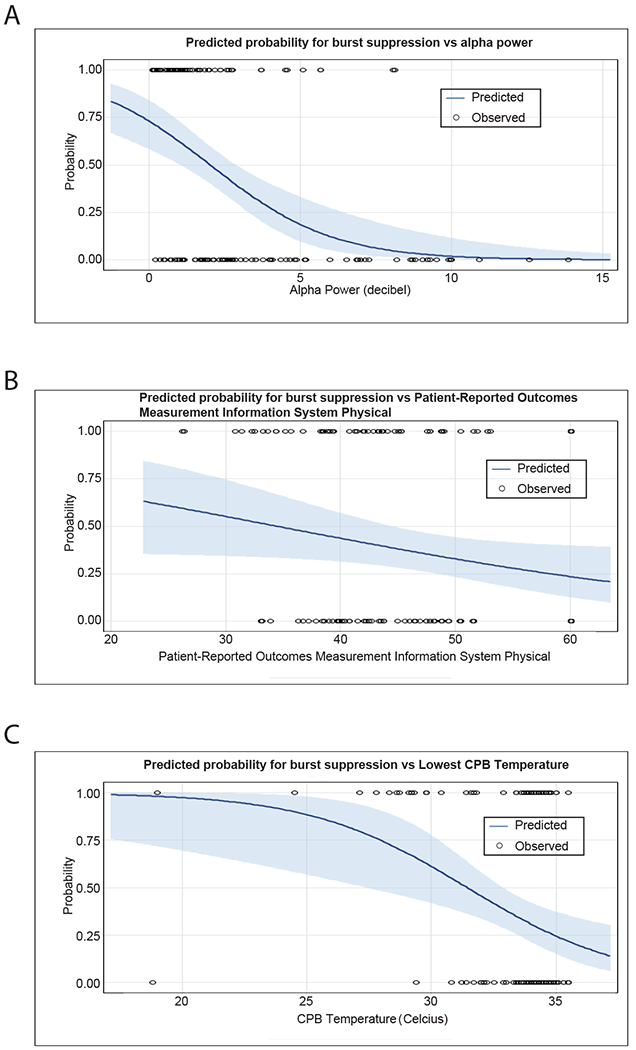
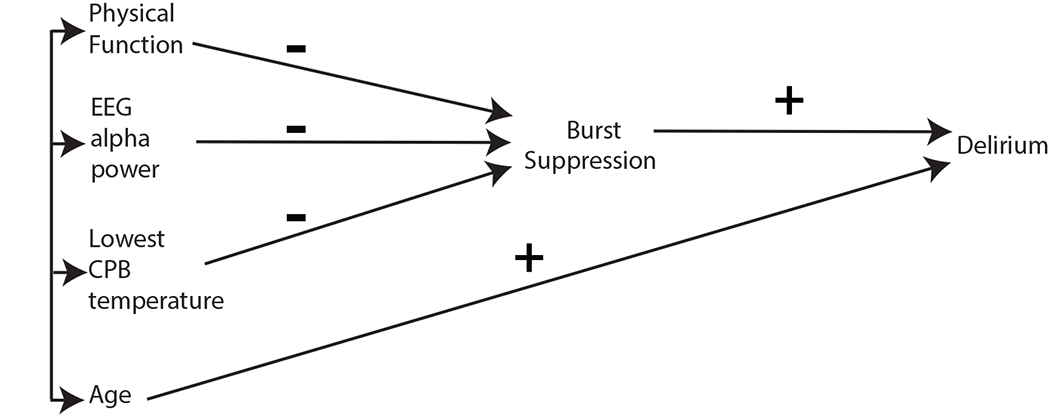
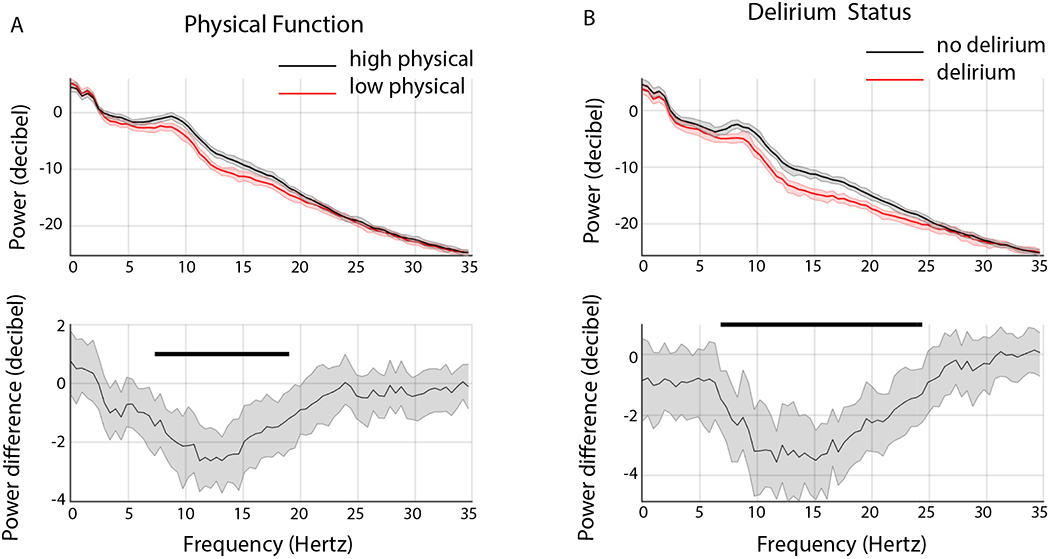
Results: The incidence of delirium in patients with CPB burst-suppression was 25% (15 of 60) compared with 6% (5 of 81) in patients without CPB burst-suppression. In univariate analyses, age (odds ratio, 1.08 [95% CI, 1.03 to 1.14]; P = 0.002), lowest CPB temperature (odds ratio, 0.79 [0.66 to 0.94]; P = 0.010), alpha power (odds ratio, 0.65 [0.54 to 0.80]; P < 0.001), and physical function (odds ratio, 0.95 [0.91 to 0.98]; P = 0.007) were associated with CPB burst-suppression. In separate univariate analyses, age (odds ratio, 1.09 [1.02 to 1.16]; P = 0.009), abbreviated Montreal Cognitive Assessment (odds ratio, 0.80 [0.66 to 0.97]; P = 0.024), alpha power (odds ratio, 0.75 [0.59 to 0.96]; P = 0.025), and CPB burst-suppression (odds ratio, 3.79 [1.5 to 9.6]; P = 0.005) were associated with delirium. However, only physical function (odds ratio, 0.96 [0.91 to 0.99]; P = 0.044), lowest CPB temperature (odds ratio, 0.73 [0.58 to 0.88]; P = 0.003), and electroencephalogram alpha power (odds ratio, 0.61 [0.47 to 0.76]; P < 0.001) were retained as predictors in the burst-suppression multivariable model. Burst-suppression (odds ratio, 4.1 [1.5 to 13.7]; P = 0.012) and age (odds ratio, 1.07 [0.99 to 1.15]; P = 0.090) were retained as predictors in the delirium multivariable model. Delirium was associated with decreased electroencephalogram power from 6.8 to 24.4 Hertz.
Conclusions: The inference from the present study is that CPB burst-suppression mediates the effects of physical function, lowest CPB temperature, and electroencephalogram alpha power on delirium.
Conflict of interest statement
Figures
Comment in
-
Burst-suppression and Postoperative Delirium: Comment.Anesthesiology. 2021 Feb 1;134(2):351-352. doi: 10.1097/ALN.0000000000003631. Anesthesiology. 2021. PMID: 33433616 No abstract available.
-
Burst-suppression and Postoperative Delirium: Reply.Anesthesiology. 2021 Feb 1;134(2):352-353. doi: 10.1097/ALN.0000000000003632. Anesthesiology. 2021. PMID: 33433617 Free PMC article. No abstract available.
Comment on
-
Postoperative Delirium: A Minefield of Markers and Mediators.Anesthesiology. 2020 Aug;133(2):255-257. doi: 10.1097/ALN.0000000000003383. Anesthesiology. 2020. PMID: 32568846 No abstract available.
References
-
- American Psychiatric Association., American Psychiatric Association DSM-5 Task Force.: Diagnostic and statistical manual of mental disorders : DSM-5, 5th edition Washington, D.C., American Psychiatric Association, 2013
-
- Inouye SK: Delirium in older persons. N Engl J Med 2006; 354: 1157–65 - PubMed
-
- Ogawa M, Izawa KP, Satomi-Kobayashi S, Kitamura A, Tsuboi Y, Komaki K, Ono R, Sakai Y, Tanaka H, Okita Y: Preoperative exercise capacity is associated with the prevalence of postoperative delirium in elective cardiac surgery. Aging Clin Exp Res 2018; 30: 27–34 - PubMed
-
- Culley DJ, Flaherty D, Fahey MC, Rudolph JL, Javedan H, Huang CC, Wright J, Bader AM, Hyman BT, Blacker D, Crosby G: Poor Performance on a Preoperative Cognitive Screening Test Predicts Postoperative Complications in Older Orthopedic Surgical Patients. Anesthesiology 2017; 127: 765–774 - PMC - PubMed
