

Characterizing heart failure with preserved and reduced ejection fraction: An imaging and plasma biomarker approach
- PMID: 32349122
- PMCID: PMC7190371
- DOI: 10.1371/journal.pone.0232280
Characterizing heart failure with preserved and reduced ejection fraction: An imaging and plasma biomarker approach
Abstract
Introduction: The pathophysiology of heart failure with preserved ejection fraction (HFpEF) remains incompletely defined. We aimed to characterize HFpEF compared to heart failure with reduced ejection fraction (HFrEF) and asymptomatic hypertensive or non-hypertensive controls.
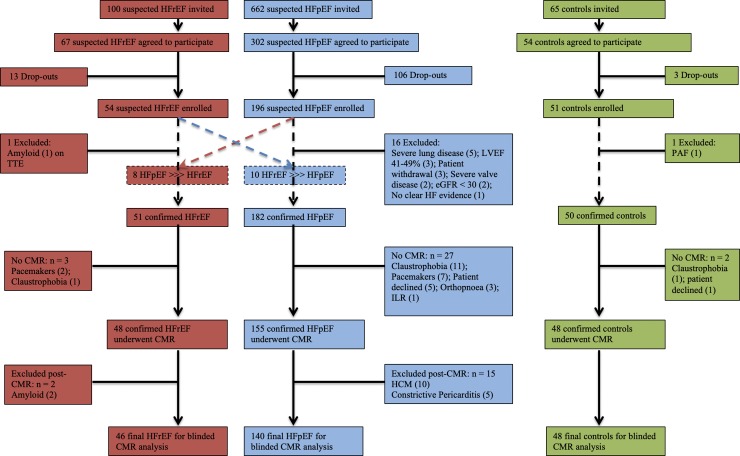
Materials and methods: Prospective, observational study of 234 subjects (HFpEF n = 140; HFrEF n = 46, controls n = 48, age 73±8, males 49%) who underwent echocardiography, cardiovascular magnetic resonance imaging (CMR), plasma biomarker analysis (panel of 22) and 6-minute walk testing (6MWT). The primary end-point was the composite of all-cause mortality and/or HF hospitalization.
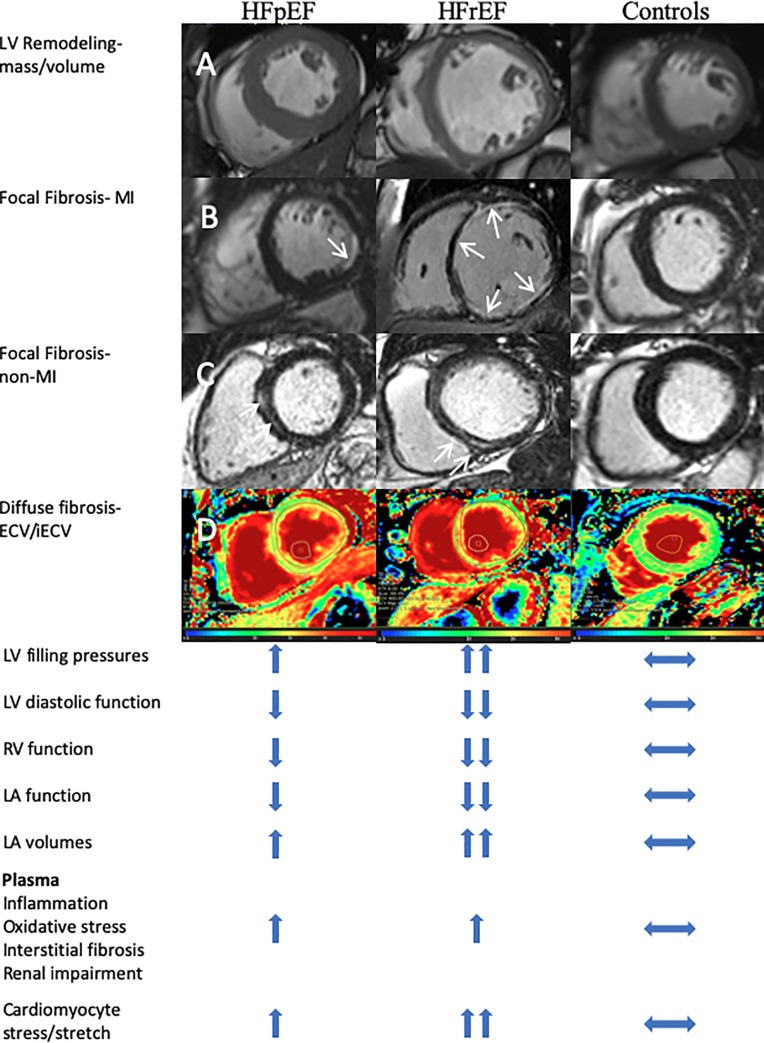
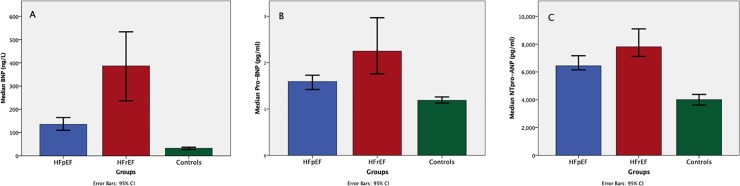
Results: Compared to controls both HF groups had lower exercise capacity, lower left ventricular (LV) EF, higher LV filling pressures (E/E', B-type natriuretic peptide [BNP], left atrial [LA] volumes), more right ventricular (RV) systolic dysfunction, more focal and diffuse fibrosis and higher levels of all plasma markers. LV remodeling (mass/volume) was different between HFpEF (concentric, 0.68±0.16) and HFrEF (eccentric, 0.47±0.15); p<0.0001. Compared to controls, HFpEF was characterized by (mild) reductions in LVEF, more myocardial fibrosis, LA remodeling/dysfunction and RV dysfunction. HFrEF patients had lower LVEF, increased LV volumes, greater burden of focal and diffuse fibrosis, more RV remodeling, lower LAEF and higher LA volumes compared to HFpEF. Inflammatory/fibrotic/renal dysfunction plasma markers were similarly elevated in both HF groups but markers of cardiomyocyte stretch/damage (BNP, pro-BNP, N-terminal pro-atrial natriuretic peptide and troponin-I) were higher in HFrEF compared to HFpEF; p<0.0001. Focal fibrosis was associated with galectin3, GDF-15, MMP-3, MMP-7, MMP-8, BNP, pro-BNP and NTproANP; p<0.05. Diffuse fibrosis was associated with GDF-15, Tenascin-C, MMP-2, MMP-3, MMP-7, BNP, proBNP and NTproANP; p<0.05. Composite event rates (median 1446 days follow-up) did not differ between HFpEF and HFrEF (Log-Rank p = 0.784).
Conclusions: HFpEF is a distinct pathophysiological entity compared to age- and sex-matched HFrEF and controls. HFpEF and HFrEF are associated with similar adverse outcomes. Inflammation is common in both HF phenotypes but cardiomyocyte stretch/stress is greater in HFrEF.
Conflict of interest statement
Authors (LZ and JY) were employed by Bristol Myers Squibb which facilitated plasma biomarker analysis. Bristol Myers Squibb did not have any additional role in the study design, data collection and analysis, decision to publish or preparation of the manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal. 2016;37(27):2129–200. 10.1093/eurheartj/ehw128 - DOI - PubMed
-
- Kanagala P, Cheng ASH, Singh A, Khan JN, Gulsin GS, Patel P, et al. Relationship Between Focal and Diffuse Fibrosis Assessed by CMR and Clinical Outcomes in Heart Failure With Preserved Ejection Fraction. JACC Cardiovascular imaging. 2019. - PubMed
-
- Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugander M, et al. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. Journal of cardiovascular magnetic resonance: official journal of the Society for Cardiovascular Magnetic Resonance. 2013;15:92. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
