

Publicly available machine learning models for identifying opioid misuse from the clinical notes of hospitalized patients
- PMID: 32349766
- PMCID: PMC7191715
- DOI: 10.1186/s12911-020-1099-y
Publicly available machine learning models for identifying opioid misuse from the clinical notes of hospitalized patients
Abstract
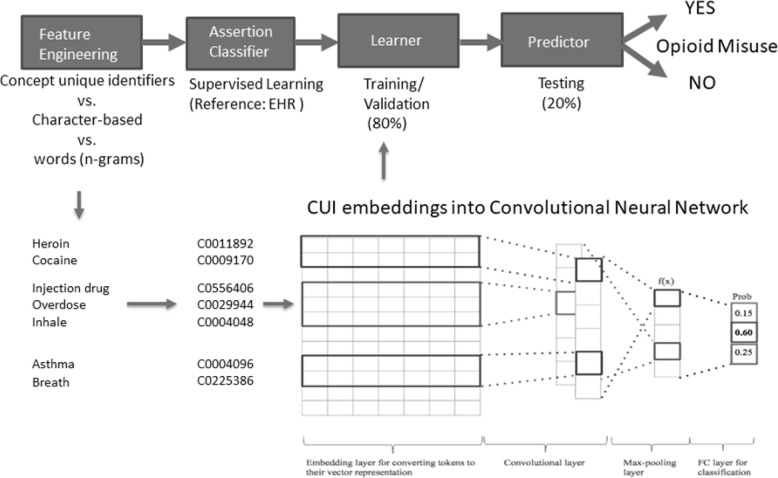
Background: Automated de-identification methods for removing protected health information (PHI) from the source notes of the electronic health record (EHR) rely on building systems to recognize mentions of PHI in text, but they remain inadequate at ensuring perfect PHI removal. As an alternative to relying on de-identification systems, we propose the following solutions: (1) Mapping the corpus of documents to standardized medical vocabulary (concept unique identifier [CUI] codes mapped from the Unified Medical Language System) thus eliminating PHI as inputs to a machine learning model; and (2) training character-based machine learning models that obviate the need for a dictionary containing input words/n-grams. We aim to test the performance of models with and without PHI in a use-case for an opioid misuse classifier.
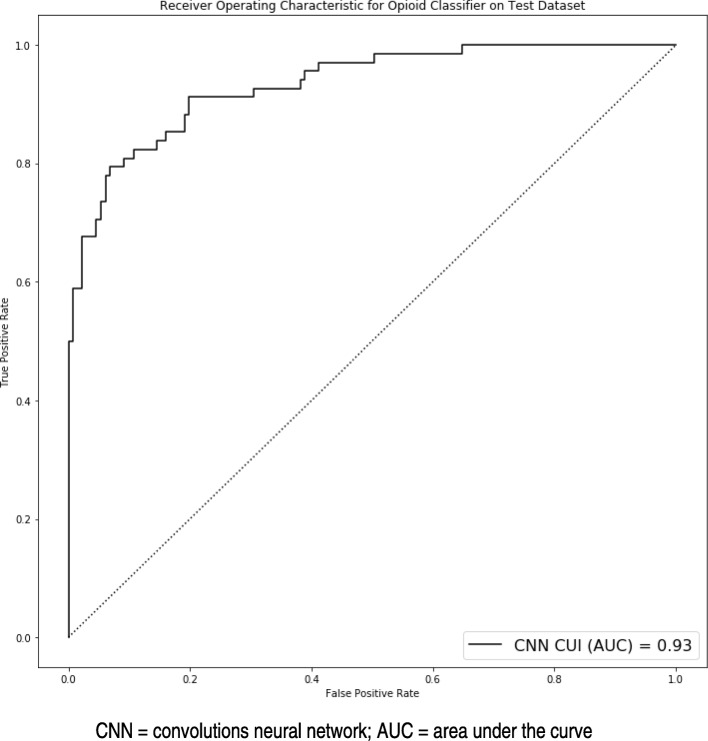
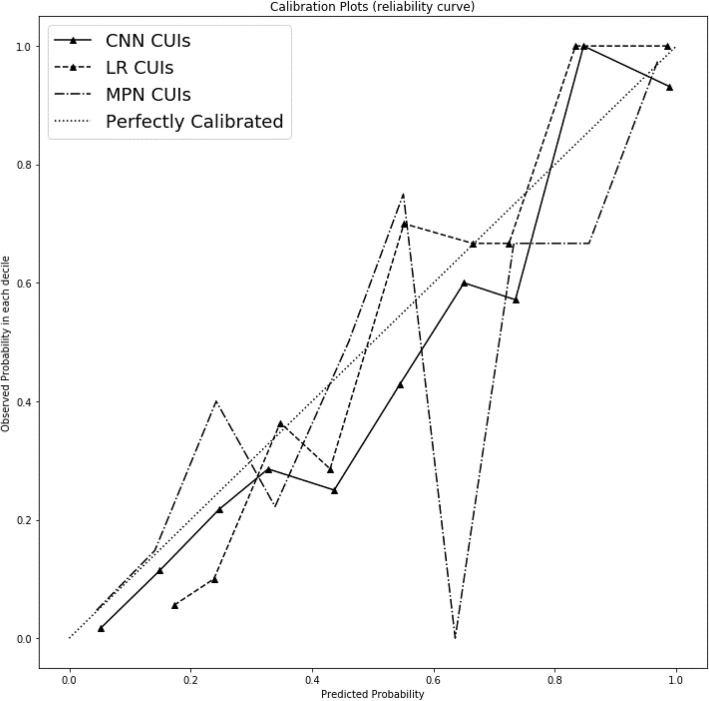
Methods: An observational cohort sampled from adult hospital inpatient encounters at a health system between 2007 and 2017. A case-control stratified sampling (n = 1000) was performed to build an annotated dataset for a reference standard of cases and non-cases of opioid misuse. Models for training and testing included CUI codes, character-based, and n-gram features. Models applied were machine learning with neural network and logistic regression as well as expert consensus with a rule-based model for opioid misuse. The area under the receiver operating characteristic curves (AUROC) were compared between models for discrimination. The Hosmer-Lemeshow test and visual plots measured model fit and calibration.
Results: Machine learning models with CUI codes performed similarly to n-gram models with PHI. The top performing models with AUROCs > 0.90 included CUI codes as inputs to a convolutional neural network, max pooling network, and logistic regression model. The top calibrated models with the best model fit were the CUI-based convolutional neural network and max pooling network. The top weighted CUI codes in logistic regression has the related terms 'Heroin' and 'Victim of abuse'.
Conclusions: We demonstrate good test characteristics for an opioid misuse computable phenotype that is void of any PHI and performs similarly to models that use PHI. Herein we share a PHI-free, trained opioid misuse classifier for other researchers and health systems to use and benchmark to overcome privacy and security concerns.
Keywords: Computable phenotype; Heroin; Machine learning; Natural language processing; Opioid misuse; Opioid use disorder.
Conflict of interest statement
The authors declare they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
