

Term complications and subsequent risk of preterm birth: registry based study
- PMID: 32349968
- PMCID: PMC7188013
- DOI: 10.1136/bmj.m1007
Term complications and subsequent risk of preterm birth: registry based study
Abstract
Objective: To explore conditions and outcomes of a first delivery at term that might predict later preterm birth.
Design: Population based, prospective register based study.
Setting: Medical Birth Registry of Norway, 1999-2015.
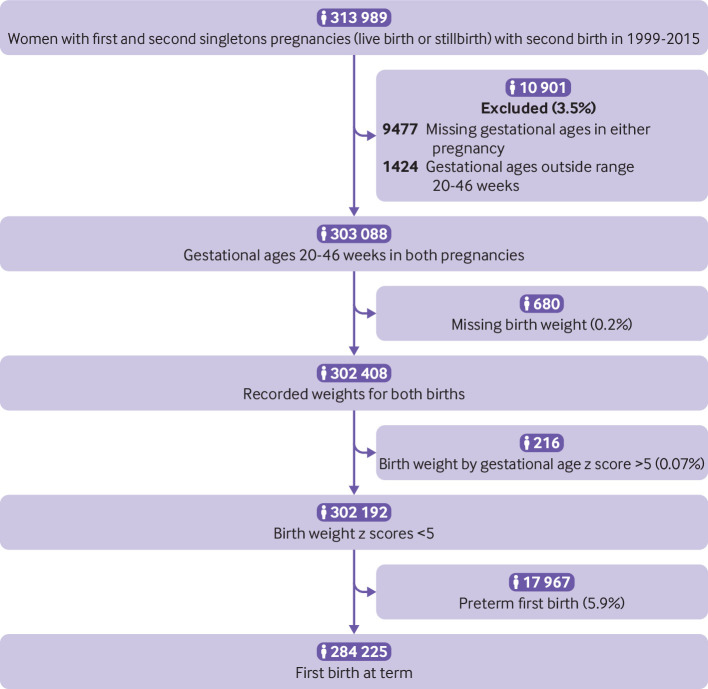
Participants: 302 192 women giving birth (live or stillbirth) to a second singleton child between 1999 and 2015.
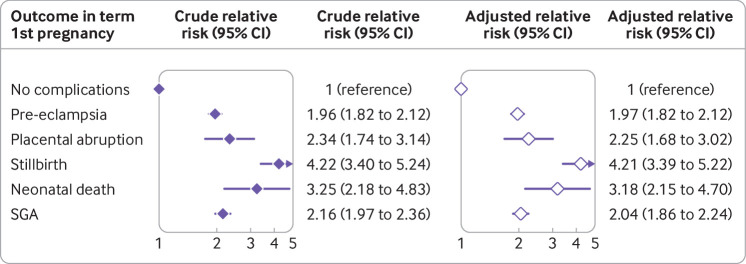
Main outcome measures: Main outcome was the relative risk of preterm delivery (<37 gestational weeks) in the birth after a term first birth with pregnancy complications: pre-eclampsia, placental abruption, stillbirth, neonatal death, and small for gestational age.
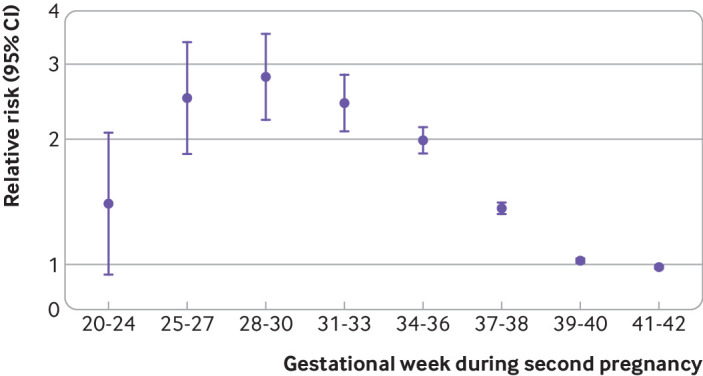
Results: Women with any of the five complications at term showed a substantially increased risk of preterm delivery in the next pregnancy. The absolute risks for preterm delivery in a second pregnancy were 3.1% with none of the five term complications (8202/265 043), 6.1% after term pre-eclampsia (688/11 225), 7.3% after term placental abruption (41/562), 13.1% after term stillbirth (72/551), 10.0% after term neonatal death (22/219), and 6.7% after term small for gestational age (463/6939). The unadjusted relative risk for preterm birth after term pre-eclampsia was 2.0 (95% confidence interval 1.8 to 2.1), after term placental abruption was 2.3 (1.7 to 3.1), after term stillbirth was 4.2 (3.4 to 5.2), after term neonatal death was 3.2 (2.2 to 4.8), and after term small for gestational age was 2.2 (2.0 to 2.4). On average, the risk of preterm birth was increased 2.0-fold (1.9-fold to 2.1-fold) with one term complication in the first pregnancy, and 3.5-fold (2.9-fold to 4.2-fold) with two or more complications. The associations persisted after excluding recurrence of the specific complication in the second pregnancy. These links between term complications and preterm delivery were also seen in the reverse direction: preterm birth in the first pregnancy predicted complications in second pregnancies delivered at term.
Conclusions: Pre-eclampsia, placental abruption, stillbirth, neonatal death, or small for gestational age experienced in a first term pregnancy are associated with a substantially increased risk of subsequent preterm delivery. Term complications seem to share important underlying causes with preterm delivery that persist from pregnancy to pregnancy, perhaps related to a mother's predisposition to disorders of placental function.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICME uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: LGK reports grants from the US-Norway Fulbright Foundation for Educational Exchange, during the conduct of the study; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical