

Utility of Procalcitonin as a Biomarker for Sepsis in Children
- PMID: 32350044
- PMCID: PMC7315022
- DOI: 10.1128/JCM.01851-19
Utility of Procalcitonin as a Biomarker for Sepsis in Children
Abstract
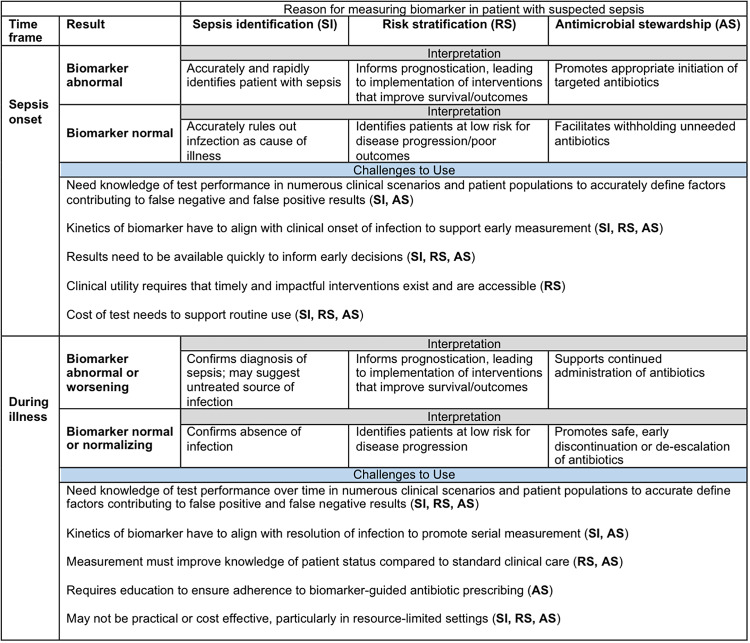
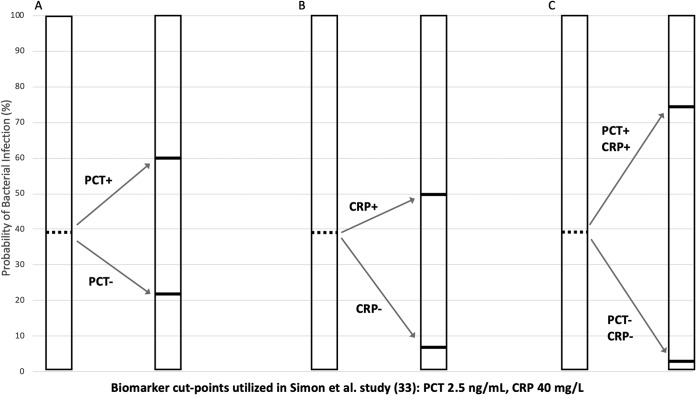
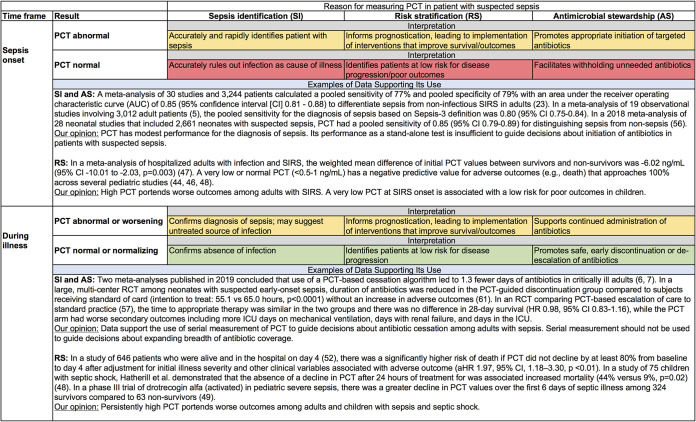
Sepsis is a complex process defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. It is associated with significant morbidity and mortality rates in both adults and children, and emphasis has been placed on its early recognition and prompt provision of antimicrobials. Owing to limitations of current diagnostic tests (i.e., poor sensitivity and delayed results), significant research has been conducted to identify sepsis biomarkers. Ideally, a biomarker could reliably and rapidly distinguish bacterial infection from other, noninfectious causes of systemic inflammatory illness. In doing so, a sepsis biomarker could be used for earlier identification of sepsis, risk stratification/prognostication, and/or guidance of antibiotic decision-making. In this minireview, we review one of the most common clinically used sepsis biomarkers, procalcitonin, and its roles in sepsis management in these three areas. We highlight key findings in the adult literature but focus the bulk of this review on pediatric sepsis. The challenges and limitations of procalcitonin measurement in sepsis are also discussed.
Keywords: adults; biomarkers; pediatrics; procalcitonin; sepsis.
Copyright © 2020 American Society for Microbiology.
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. 2016. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 315:801–810. doi:10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, Colombara DV, Ikuta KS, Kissoon N, Finfer S, Fleischmann-Struzek C, Machado FR, Reinhart KK, Rowan K, Seymour CW, Watson RS, West TE, Marinho F, Hay SI, Lozano R, Lopez AD, Angus DC, Murray CJL, Naghavi M. 2020. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet 395:200–211. doi:10.1016/S0140-6736(19)32989-7. - DOI - PMC - PubMed
-
- Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, Kadri SS, Angus DC, Danner RL, Fiore AE, Jernigan JA, Martin GS, Septimus E, Warren DK, Karcz A, Chan C, Menchaca JT, Wang R, Gruber S, Klompas M. 2017. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009–2014. JAMA 318:1241–1249. doi:10.1001/jama.2017.13836. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
