

Scheduling nab-paclitaxel combined with gemcitabine as first-line treatment for metastatic pancreatic adenocarcinoma
- PMID: 32350413
- PMCID: PMC7283477
- DOI: 10.1038/s41416-020-0846-2
Scheduling nab-paclitaxel combined with gemcitabine as first-line treatment for metastatic pancreatic adenocarcinoma
Abstract
Background: Nab-paclitaxel plus gemcitabine (nabP+gemcitabine) offers modest survival gains for patients with metastatic pancreatic ductal adenocarcinoma (PDAC). Sequential scheduling of nabP+gemcitabine in a PDAC mouse model improved efficacy; this hypothesis was tested in a clinical trial.
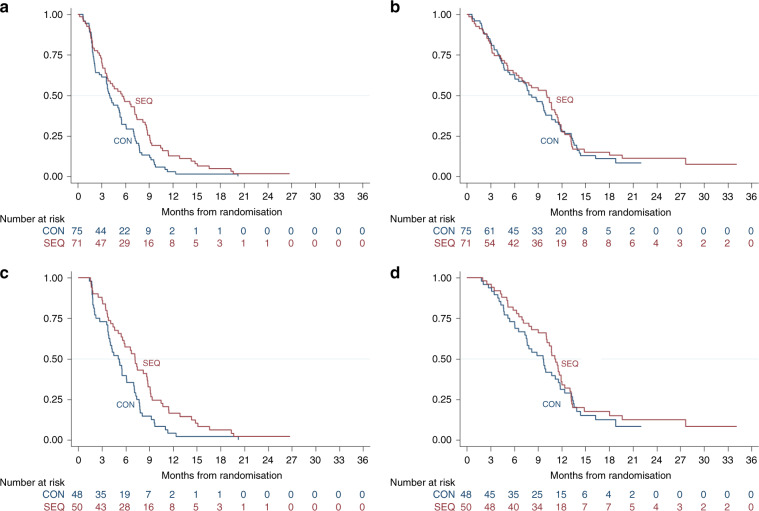
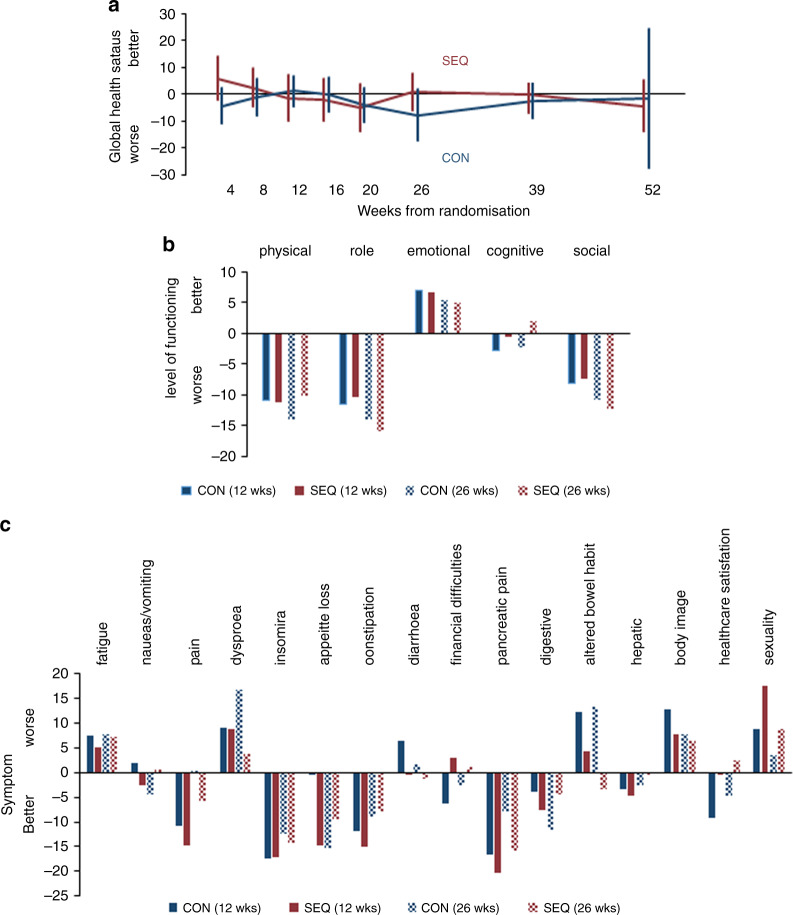
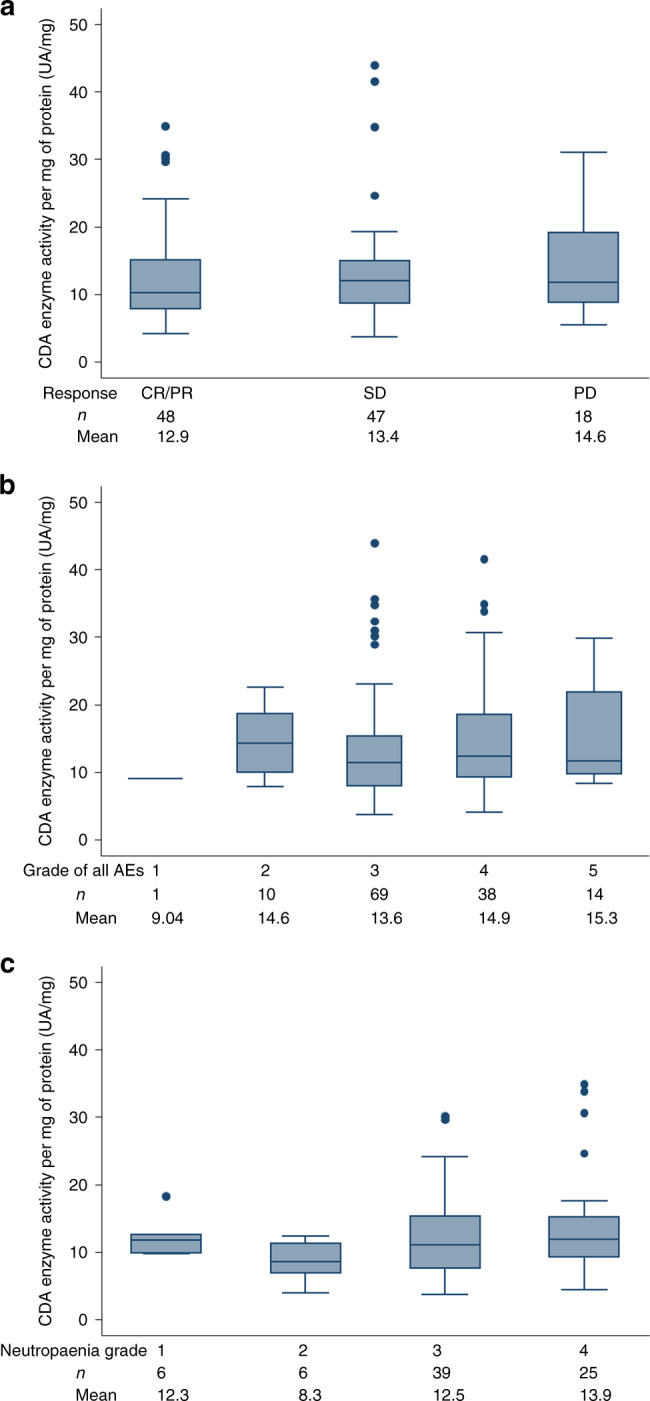
Methods: Patients with previously untreated metastatic PDAC were randomised to receive nabP+gemcitabine administered either concomitantly on the same day, or sequentially, with gemcitabine administered 24 h after nabP. The primary outcome measure was progression-free survival (PFS). Secondary outcome measures were objective response rate (ORR), overall survival (OS), safety, quality of life (QoL) and predictive biomarkers.
Results: In total, 71 patients received sequential (SEQ) and 75 concomitant (CON) treatment. Six-month PFS was 46% with SEQ and 32% with CON scheduling. Median PFS (5.6 versus 4.0 months, hazard ratio [HR] 0.67, 95% confidence interval [95% CI] 0.47-0.95, p = 0.022) and ORR (52% versus 31%, p = 0.023) favoured the SEQ arm; median OS was 10.2 versus 8.2 months (HR 0.93, 95% CI 0.65-1.33, p = 0.70). CTCAE Grade ≥3 neutropaenia incidence doubled with SEQ therapy but was not detrimental to QoL. Strongly positive tumour epithelial cytidine deaminase (CDA) expression favoured benefit from SEQ therapy (PFS HR 0.31, 95% CI 0.13-0.70).
Conclusions: SEQ delivery of nabP+gemcitabine improved PFS and ORR, with manageable toxicity, but did not significantly improve OS.
Clinical trial registration: ISRCTN71070888; ClinialTrials.gov (NCT03529175).
Conflict of interest statement
The following conflicts of interest are declared, which were incurred during the conduct of the SIEGE: Dr Corrie was the lead recipient of the SIEGE research grant from Celgene, which was paid to Cambridge University NHS Foundation Trust. Dr Basu and Dr Propper received funding from Celgene for research work outside of the SIEGE trial. Professor Bridgewater, Dr Corrie, Professor Evans, Professor Palmer, Professor Wadsley and Dr Wassan report personal fees from Celgene for advisory boards and/or speaker fees. Dr Falk, Professor Valle and Dr Basu received a travel grant from Celgene. Dr Propper was an expert witness when nab-Paclitaxel was submitted for NICE evaluation in 2017. Professor Evans is an editor of the clinical subject section of the
Figures
References
-
- Goldstein D, El-Maraghi RH, Hammel P, Heinemann V, Kunzmann V, Sastre J, et al. Nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: long-term survival from a phase III trial. J. Natl Cancer Inst. 2015;107:3–10. - PubMed
