

Survey results of 3D-CRT and IMRT quality assurance practice
- PMID: 32351006
- PMCID: PMC7386182
- DOI: 10.1002/acm2.12885
Survey results of 3D-CRT and IMRT quality assurance practice
Abstract
Purpose: To create a snapshot of common practices for 3D-CRT and intensity-modulated radiation therapy (IMRT) QA through a large-scale survey and compare to TG-218 recommendations.
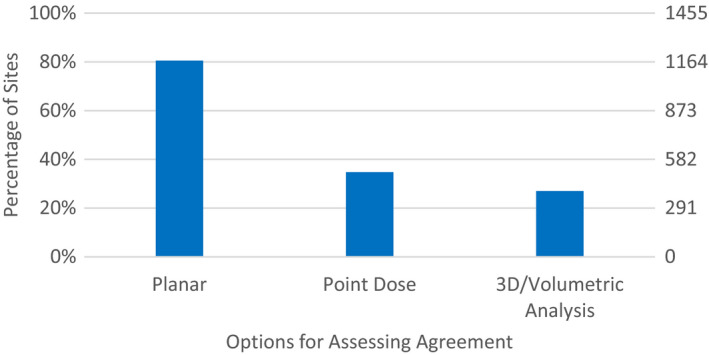
Methods: A survey of 3D-CRT and IMRT QA was constructed at and distributed by the IROC-Houston QA center to all institutions monitored by IROC (n = 2,861). The first part of the survey asked about methods to check dose delivery for 3D-CRT. The bulk of the survey focused on IMRT QA, inquiring about treatment modalities, standard tools used to verify planned dose, how assessment of agreement is calculated and the comparison criteria used, and the strategies taken if QA fails.
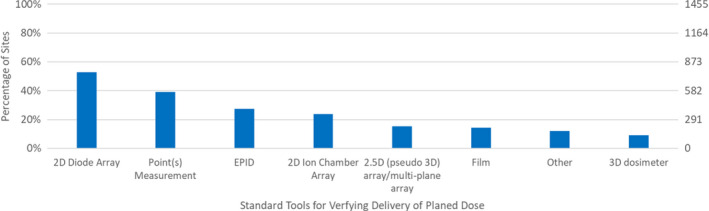
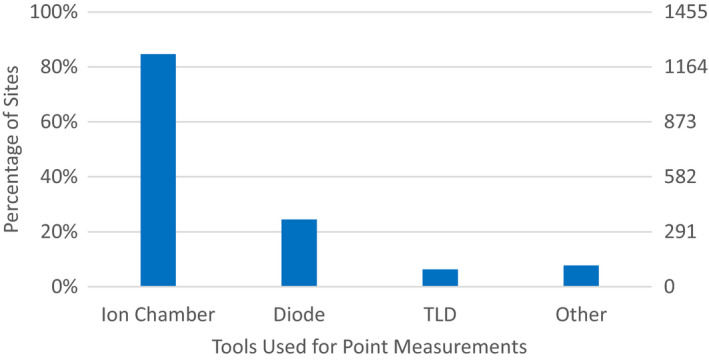
Results: The most common tools for dose verification were a 2D diode array (52.8%), point(s) measurement (39.0%), EPID (27.4%), and 2D ion chamber array (23.9%). When IMRT QA failed, the highest average rank strategy utilized was to remeasure with the same setup, which had an average position ranking of 1.1 with 90.4% of facilities employing this strategy. The second highest average ranked strategy was to move to a new calculation point and remeasure (54.9%); this had an average ranking of 2.1.
Conclusion: The survey provided a snapshot of the current state of dose verification for IMRT radiotherapy. The results showed variability in approaches and that work is still needed to unify and tighten criteria in the medical physics community, especially in reference to TG-218's recommendations.
Keywords: IMRT QA; TG-218; dose verification; patient specific QA; survey.
© 2020 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflicts of interests to declare.
Figures
References
-
- Valdes G, Scheuermann R, Hung C, Olszanski A, Bellerive M, Solberg T. A mathematical framework for virtual IMRT QA using machine learning. Med Phys. 2016;43:4323–4334. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
