

Total Mesorectal Excision Technique-Past, Present, and Future
- PMID: 32351336
- PMCID: PMC7188504
- DOI: 10.1055/s-0039-3402776
Total Mesorectal Excision Technique-Past, Present, and Future
Abstract
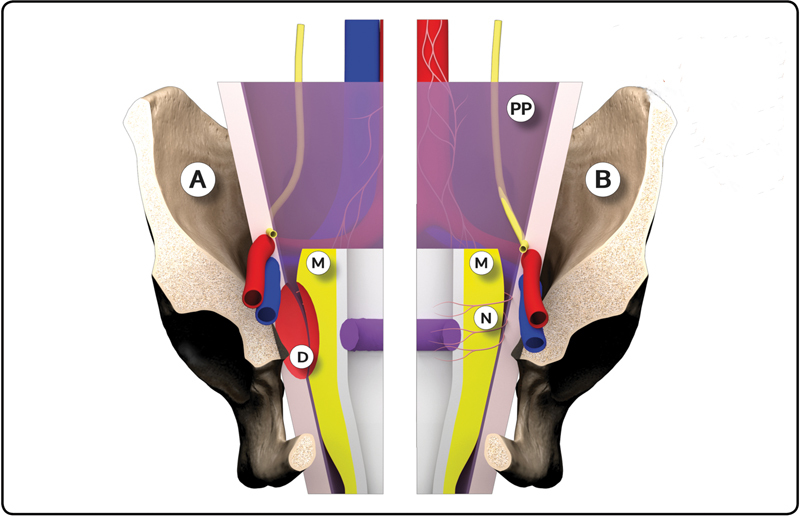
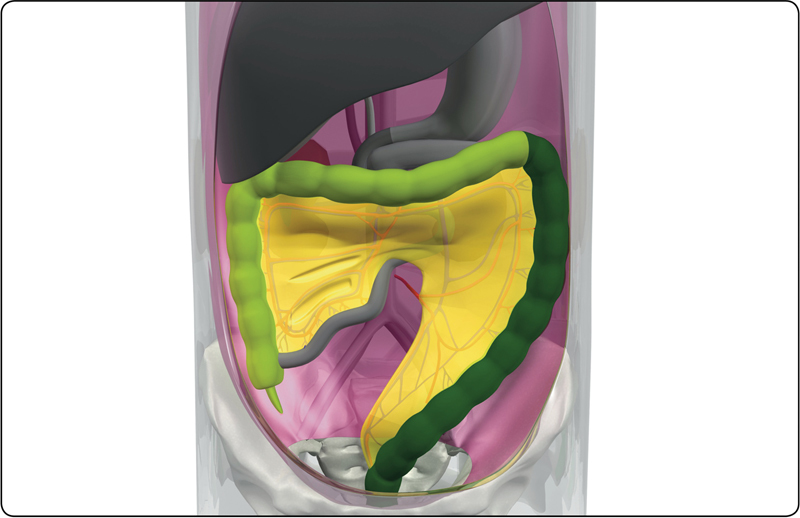
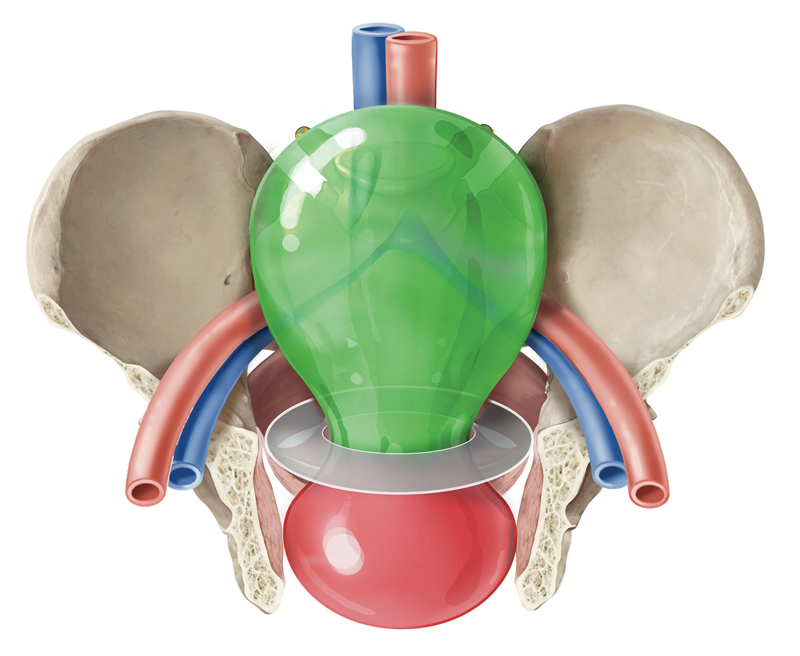
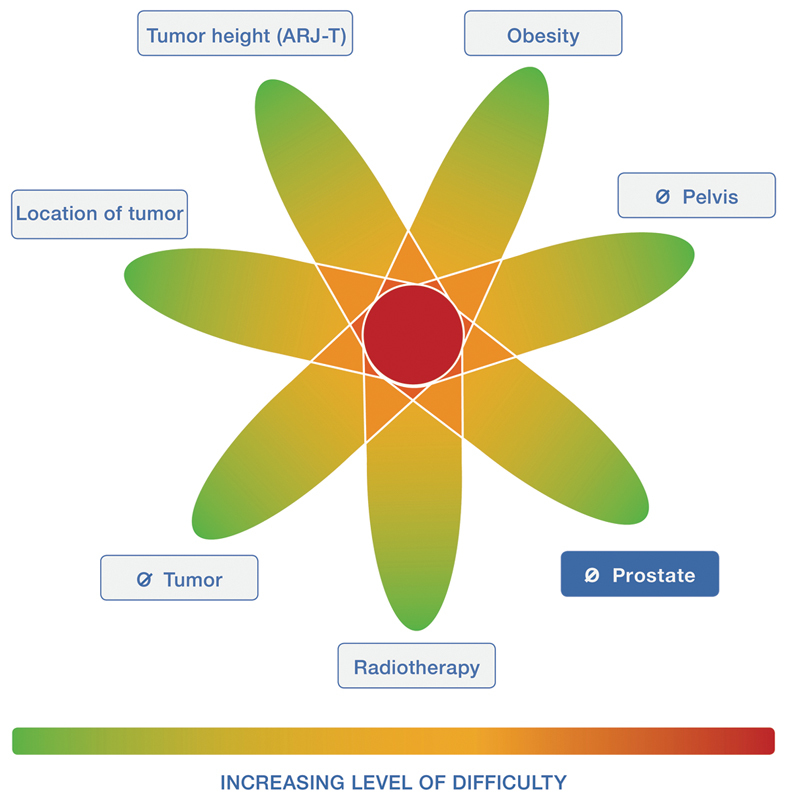
While the treatment of rectal cancer is multimodal, above all, a proper oncological resection is critical. The surgical management of rectal cancer has substantially evolved over the past 100 years, and continues to progress as we seek the best treatment. Rectal cancer was historically an unsurvivable disease, with poor understanding of the embryological planes, lymphatic drainage, and lack of standardized technique. Major improvements in recurrence, survival, and quality of life have resulted from advances in preoperative staging, pathologic assessment, the development and timing of multimodal therapies, and surgical technique. The most significant contribution in advancing rectal cancer care may be the standardization and widespread implementation of total mesorectal excision (TME). The TME, popularized by Professor Heald in the early 1980s as a sharp, meticulous dissection of the tumor and mesorectum with all associated lymph nodes through the avascular embryologic plane, has shown universal reproducible reductions in local recurrence and improvement in disease-free and overall survival. Widespread education and training of surgeons worldwide in the TME have significantly impact outcomes for rectal cancer surgery, and the procedure has become the gold standard for curative resection of rectal cancer. In this article, we discuss the evolution of the standard abdominal approach to the TME, with emphasis on the history, relevant anatomy, standard procedure steps, oncologic outcomes, and technical evolution.
Keywords: holy plane; mesorectal fascia; rectal cancer; total mesorectal excision (TME); transanal total mesorectal excision (TaTME).
© Thieme Medical Publishers.
Conflict of interest statement
Conflict of Interest None declared.
Figures
References
-
- Miles W E. A method of performing abdomino-perineal excision for carcinoma of the rectum and of the terminal portion of the pelvic colon. Lancet. 1908;2:1812–1813. - PubMed
-
- Miles W E. A method of performing abdomino-perineal excision for carcinoma of the rectum and of the terminal portion of the pelvic colon (1908) CA Cancer J Clin. 1971;21(06):361–364. - PubMed
-
- Miles W E. The radical abdomino-perineal operation for cancer of the pelvic colon. BMJ. 1910;11:941–943.
-
- Moynihan B GA. The surgical treatment of cancer of the sigmoid flexure and rectum with special reference to the principles to be observed. Surg Gynecol Obstet. 1908;6:463–468.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
