

Hypertensive Disorders of Pregnancy and Future Cardiovascular Health
- PMID: 32351977
- PMCID: PMC7174679
- DOI: 10.3389/fcvm.2020.00059
Hypertensive Disorders of Pregnancy and Future Cardiovascular Health
Abstract
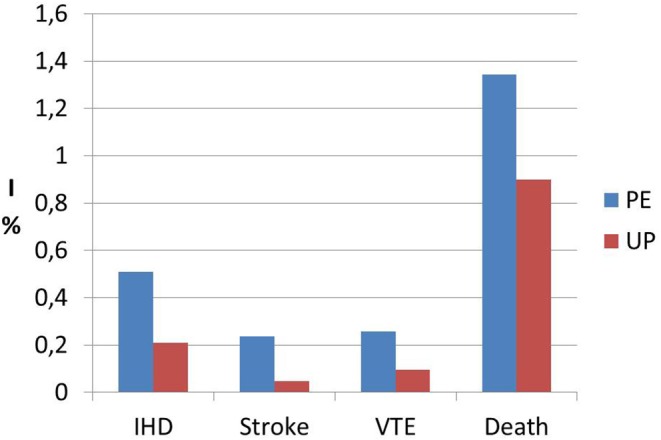
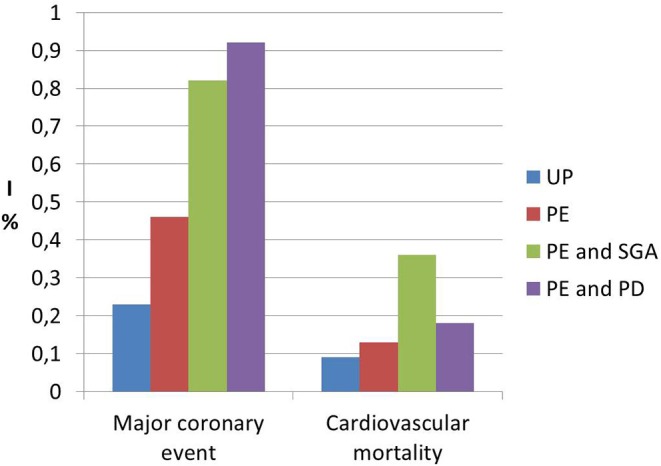
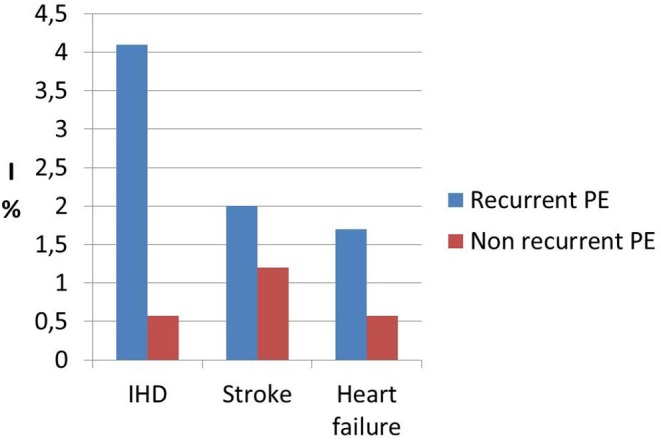
Hypertensive disorders of pregnancy (HDP) occur in almost 10% of gestations. These women are known to have higher cardiovascular morbidity and mortality later in life in comparison with parous controls who had normotensive pregnancies. Several studies have demonstrated that women with preeclampsia present in a state of segmental impaired myocardial function, biventricular chamber dysfunction, adverse biventricular remodeling, and hypertrophy, a compromised hemodynamic state and indirect echocardiographic signs of localized myocardial ischemia and fibrosis. These cardiac functional and geometric changes are known to have strong predictive value for cardiovascular disease in non-pregnant subjects. A "dose effect" response seems to regulate this relationship with severe HDP, early-onset HDP, coexistence of fetal growth disorders, and recurrence of HDP resulting in poorer cardiovascular measures. The mechanism underlying the relationship between HDP in younger women and cardiovascular disease later in life is unclear but could be explained by sharing of pre-pregnancy cardiovascular risk factors or due to a direct impact of HDP on the maternal cardiovascular system conferring a state of increased susceptibility to future metabolic or hemodynamic insults. If so, the prevention of HDP itself would become all the more urgent. Shortly after delivery, women who experienced HDP express an increased risk of classic cardiovascular risk factors such as essential hypertension, renal disease, abnormal lipid profile, and diabetes with higher frequency than controls. Within one or two decades after delivery, this group of women are more likely to experience premature cardiovascular events, such as symptomatic heart failure, myocardial ischemia, and cerebral vascular disease. Although there is general agreement that women who suffered from HDP should undertake early screening for cardiovascular risk factors in order to allow for appropriate prevention, the exact timing and modality of screening has not been standardized yet. Our findings suggest that prevention should start as early as possible after delivery by making the women aware of their increased cardiovascular risk and encouraging weight control, stop smoking, healthy diet, and daily exercise which are well-established and cost-effective prevention strategies.
Keywords: cardiovascular disease; coronary artery disease; essential hypertension; gestational hypertension; heart failure; hypertensive disorders of pregnancy; preeclampsia.
Copyright © 2020 Melchiorre, Thilaganathan, Giorgione, Ridder, Memmo and Khalil.
Figures
References
-
- Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. (2007) 335:974. 10.1136/bmj.39335.385301.BE - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical