

Utilization and Cost of an Employer-Sponsored Comprehensive Primary Care Delivery Model
- PMID: 32352529
- PMCID: PMC7193330
- DOI: 10.1001/jamanetworkopen.2020.3803
Utilization and Cost of an Employer-Sponsored Comprehensive Primary Care Delivery Model
Abstract
Importance: Primary care is increasingly delivered at or near workplaces, yet utilization and cost of employer-sponsored primary care services remain unknown.
Objective: To compare the health care utilization and cost of an employer-sponsored on-site, near-site, and virtual comprehensive primary care service delivery model with those of traditional community-based primary care.
Design, setting, and participants: This population-based cohort study of 23 518 commercially insured employees and dependents of an engineering and manufacturing firm headquartered in southern California was performed from January 1, 2016, to July 1, 2019. A subset of the population with most (≥50%) primary care visits through employer-sponsored on-site, near-site, or virtual care clinics was matched to a subset not having most such visits through the employer-sponsored clinics using propensity score matching (n = 1983 each). In sensitivity analyses, employees were matched to dependents at neighboring firms that lacked access to the employer-sponsored primary care delivery model (additional n = 1680).
Exposures: Integrated primary care, mental health, and physical therapy delivered through on-site, near-site, and virtual clinics.
Main outcomes and measures: Utilization (inpatient, outpatient, emergency department, pharmaceutical, radiology, and laboratory visits per 1000 member-months) and spending (2019 costs per member per month in US dollars) by service type.
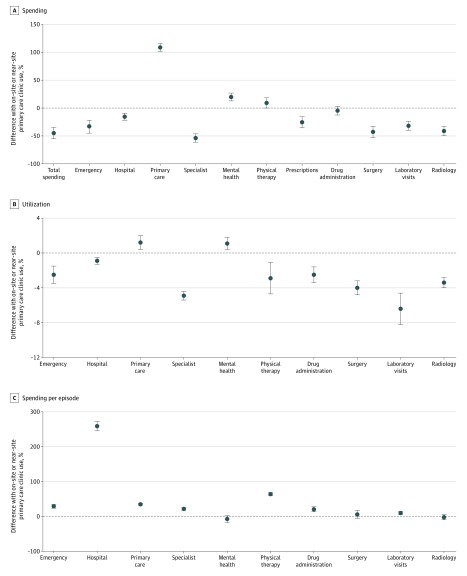
Results: A total of 23 518 individuals (mean [SD] age, 27 [15] years; 14 604 [62.1%] male) were included in the full population sample and had been enrolled in the employer-sponsored health plan for a mean of 29 months (interquartile range, 14-48 months). Of eligible members, 5292 (22.5%) used the employer-sponsored services, with 2305 (9.8%) using them for most of their primary care. The mean (SD) cost of employer-sponsored service delivery was $87 ($32) per member month. Among the matched populations (mean [SD] age, 31 [11] years; 3349 [84.5%] male) of primary users vs control individuals, total spending was 45% lower per member per month (95% CI, 35%-55%; cost difference, -$167 per member per month; 95% CI, -$204 to -$130; P < .001) among users after adjustment. The lower spending was associated with lower spending on non-primary care services, such as emergency department (-33%; 95% CI, -44% to -22%) and hospital visits (-16%; 95% CI, -22% to -10%), despite higher spending on primary care (109%; 95% CI, 102%-116%) and mental health (20%; 95% CI, 13%-27%).
Conclusions and relevance: The findings suggest that individuals who used the models' services for most of their primary care had lower total spending despite higher primary care spending, which may be associated with self-selection of lower-risk persons to the employer-sponsored services and/or with the use of comprehensive primary care.
Conflict of interest statement
Figures
References
-
- Institute of Medicine (US) Committee on the Future of Primary Care . Donaldson MS, Yordy KD, Lohr KN, Vanselow NA. Defining primary care. In: Primary Care: America’s Health in a New Era. National Academies Press (US); 1996. Accessed August 9, 2019. https://www.ncbi.nlm.nih.gov/books/NBK232631/ - PubMed
-
- Intensive Outpatient Care Program . A care model for the medically complex piloted by employers—DRIVE. Published September 25, 2017. Accessed September 23, 2019. https://www.commonwealthfund.org/publications/case-study/2017/sep/intens...
MeSH terms
LinkOut - more resources
Full Text Sources
