

Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies
- PMID: 32353039
- PMCID: PMC7192386
- DOI: 10.1371/journal.pmed.1003100
Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies
Abstract
Background: Non-alcoholic fatty liver disease (NAFLD) is a leading cause of chronic liver disease worldwide. Many individuals have risk factors associated with NAFLD, but the majority do not develop advanced liver disease: cirrhosis, hepatic decompensation, or hepatocellular carcinoma. Identifying people at high risk of experiencing these complications is important in order to prevent disease progression. This review synthesises the evidence on metabolic risk factors and their potential to predict liver disease outcomes in the general population at risk of NAFLD or with diagnosed NAFLD.
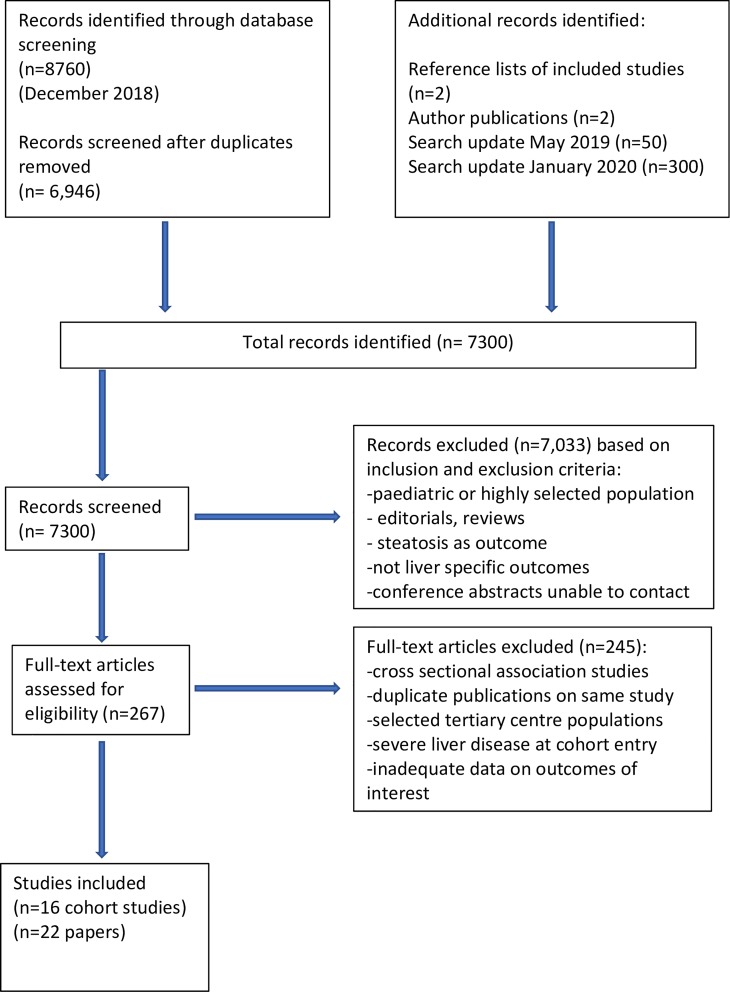
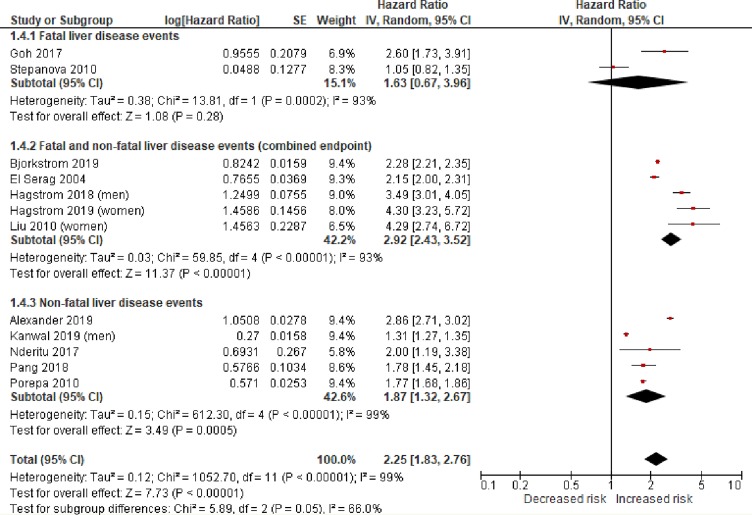
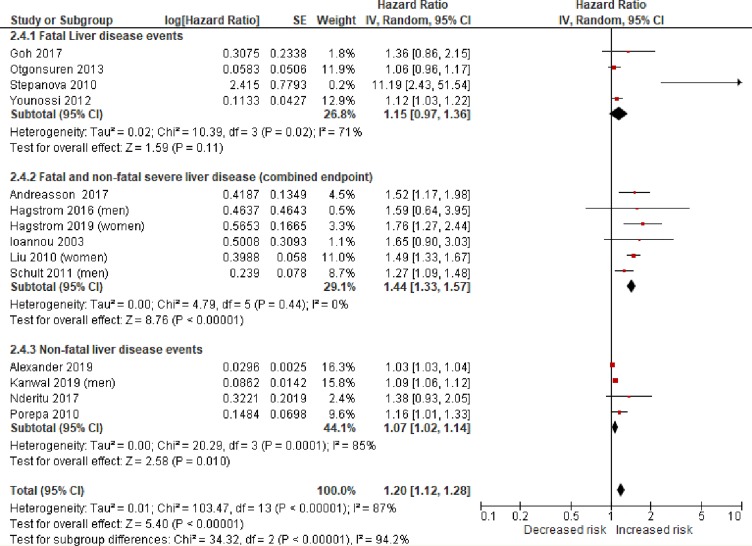
Methods and findings: We conducted a systematic review and meta-analysis of population-based cohort studies. Databases (including MEDLINE, EMBASE, the Cochrane Library, and ClinicalTrials.gov) were searched up to 9 January 2020. Studies were included that reported severe liver disease outcomes (defined as liver cirrhosis, complications of cirrhosis, or liver-related death) or advanced fibrosis/non-alcoholic steatohepatitis (NASH) in adult individuals with metabolic risk factors, compared with individuals with no metabolic risk factors. Cohorts selected on the basis of a clinically indicated liver biopsy were excluded to better reflect general population risk. Risk of bias was assessed using the QUIPS tool. The results of similar studies were pooled, and overall estimates of hazard ratio (HR) were obtained using random-effects meta-analyses. Of 7,300 unique citations, 22 studies met the inclusion criteria and were of sufficient quality, with 18 studies contributing data suitable for pooling in 2 random-effects meta-analyses. Type 2 diabetes mellitus (T2DM) was associated with an increased risk of incident severe liver disease events (adjusted HR 2.25, 95% CI 1.83-2.76, p < 0.001, I2 99%). T2DM data were from 12 studies, with 22.8 million individuals followed up for a median of 10 years (IQR 6.4 to 16.9) experiencing 72,792 liver events. Fourteen studies were included in the meta-analysis of obesity (BMI > 30 kg/m2) as a prognostic factor, providing data on 19.3 million individuals followed up for a median of 13.8 years (IQR 9.0 to 19.8) experiencing 49,541 liver events. Obesity was associated with a modest increase in risk of incident severe liver disease outcomes (adjusted HR 1.20, 95% CI 1.12-1.28, p < 0.001, I2 87%). There was also evidence to suggest that lipid abnormalities (low high-density lipoprotein and high triglycerides) and hypertension were both independently associated with incident severe liver disease. Significant study heterogeneity observed in the meta-analyses and possible under-publishing of smaller negative studies are acknowledged to be limitations, as well as the potential effect of competing risks on outcome.
Conclusions: In this review, we observed that T2DM is associated with a greater than 2-fold increase in the risk of developing severe liver disease. As the incidence of diabetes and obesity continue to rise, using these findings to improve case finding for people at high risk of liver disease will allow for effective management to help address the increasing morbidity and mortality from liver disease.
Trial registration: PROSPERO CRD42018115459.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: QMA is coordinator of the LITMUS (Liver Investigation: Testing Biomarker Utility in Steatohepatitis) consortium funded by the IMI2 H2020 Framework Program of the European Union under Grant Agreement 777377; has been a consultant for 89Bio, Abbott Laboratories, Acuitas Medical, Allergan/Tobira, Altimmune, AstraZeneca, Axcella, Blade, BMS, BNN Cardio, Celgene, Cirius, CymaBay, EcoR1, E3Bio, Eli Lilly & Company Ltd., Galmed, Genentech, Genfit SA, Gilead, Grunthal, HistoIndex, Indalo, Imperial Innovations, Intercept Pharma Europe Ltd., Inventiva, IQVIA, Janssen, Madrigal, MedImmune, Metacrine, NewGene, NGMBio, North Sea Therapeutics, Novartis, Novo Nordisk A/S, Pfizer Ltd., Poxel, ProSciento, Raptor Pharma, Servier, Terns, Viking Therapeutics; and has received research support from Abbvie, Allergan/Tobira, AstraZeneca, GlaxoSmithKline, Glympse Bio, Novartis Pharma AG, Pfizer Ltd., Vertex. The other authors have declared that no competing interests exist.
Figures
References
-
- European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–402. 10.1016/j.jhep.2015.11.004 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
