

Frequency and management of maternal infection in health facilities in 52 countries (GLOSS): a 1-week inception cohort study
- PMID: 32353314
- PMCID: PMC7196885
- DOI: 10.1016/S2214-109X(20)30109-1
Frequency and management of maternal infection in health facilities in 52 countries (GLOSS): a 1-week inception cohort study
Abstract
Background: Maternal infections are an important cause of maternal mortality and severe maternal morbidity. We report the main findings of the WHO Global Maternal Sepsis Study, which aimed to assess the frequency of maternal infections in health facilities, according to maternal characteristics and outcomes, and coverage of core practices for early identification and management.
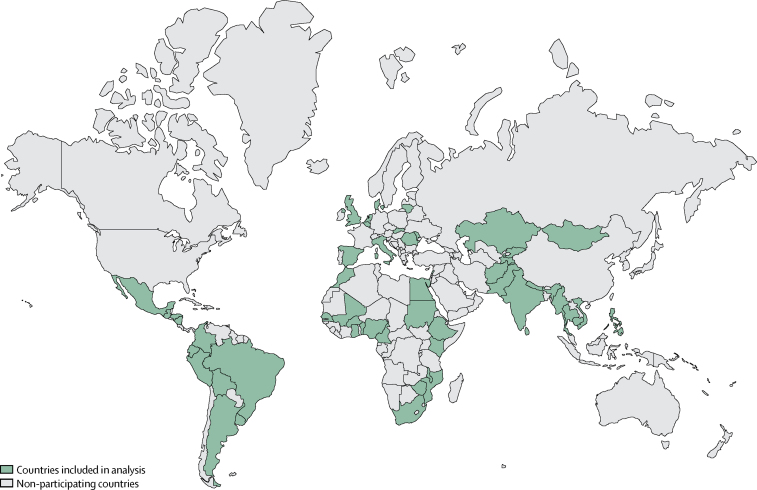
Methods: We did a facility-based, prospective, 1-week inception cohort study in 713 health facilities providing obstetric, midwifery, or abortion care, or where women could be admitted because of complications of pregnancy, childbirth, post-partum, or post-abortion, in 52 low-income and middle-income countries (LMICs) and high-income countries (HICs). We obtained data from hospital records for all pregnant or recently pregnant women hospitalised with suspected or confirmed infection. We calculated ratios of infection and infection-related severe maternal outcomes (ie, death or near-miss) per 1000 livebirths and the proportion of intrahospital fatalities across country income groups, as well as the distribution of demographic, obstetric, clinical characteristics and outcomes, and coverage of a set of core practices for identification and management across infection severity groups.
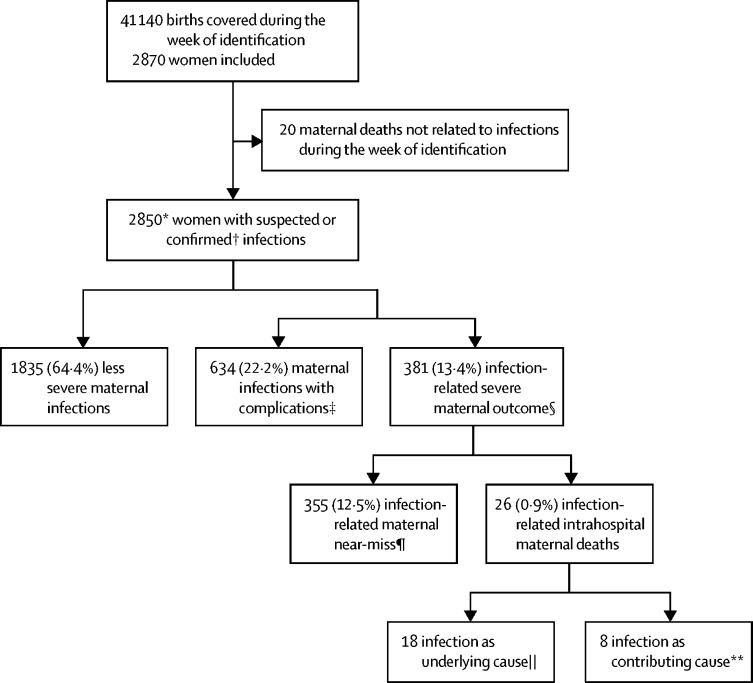
Findings: Between Nov 28, 2017, and Dec 4, 2017, of 2965 women assessed for eligibility, 2850 pregnant or recently pregnant women with suspected or confirmed infection were included. 70·4 (95% CI 67·7-73·1) hospitalised women per 1000 livebirths had a maternal infection, and 10·9 (9·8-12·0) women per 1000 livebirths presented with infection-related (underlying or contributing cause) severe maternal outcomes. Highest ratios were observed in LMICs and the lowest in HICs. The proportion of intrahospital fatalities was 6·8% among women with severe maternal outcomes, with the highest proportion in low-income countries. Infection-related maternal deaths represented more than half of the intrahospital deaths. Around two-thirds (63·9%, n=1821) of the women had a complete set of vital signs recorded, or received antimicrobials the day of suspicion or diagnosis of the infection (70·2%, n=1875), without marked differences across severity groups.
Interpretation: The frequency of maternal infections requiring management in health facilities is high. Our results suggest that contribution of direct (obstetric) and indirect (non-obstetric) infections to overall maternal deaths is greater than previously thought. Improvement of early identification is urgently needed, as well as prompt management of women with infections in health facilities by implementing effective evidence-based practices.
Funding: UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction, WHO, Merck for Mothers, and United States Agency for International Development.
Copyright © 2020 This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Say L, Chou D, Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
-
- Souza JP, Gülmezoglu AM, Vogel J. Moving beyond essential interventions for reduction of maternal mortality (the WHO Multicountry Survey on Maternal and Newborn Health): a cross-sectional study. Lancet. 2013;381:1747–1755. - PubMed
-
- Global Maternal and Neonatal Sepsis Initiative Working Group The Global Maternal and Neonatal Sepsis Initiative: a call for collaboration and action by 2030. Lancet Glob Health. 2017;5:e390–e391. - PubMed
-
- WHO . World Health Organization; Geneva, Switzerland: 2012. The WHO application of ICD-10 to deaths during pregnancy, childbirth and puerperium: ICD MM.https://apps.who.int/iris/bitstream/handle/10665/70929/9789241548458_eng...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
