

Fluid Response Evaluation in Sepsis Hypotension and Shock: A Randomized Clinical Trial
- PMID: 32353418
- PMCID: PMC9490557
- DOI: 10.1016/j.chest.2020.04.025
Fluid Response Evaluation in Sepsis Hypotension and Shock: A Randomized Clinical Trial
Abstract
Background: Fluid and vasopressor management in septic shock remains controversial. In this randomized controlled trial, we evaluated the efficacy of dynamic measures (stroke volume change during passive leg raise) to guide resuscitation and improve patient outcome.
Research question: Will resuscitation that is guided by dynamic assessments of fluid responsiveness in patients with septic shock improve patient outcomes?
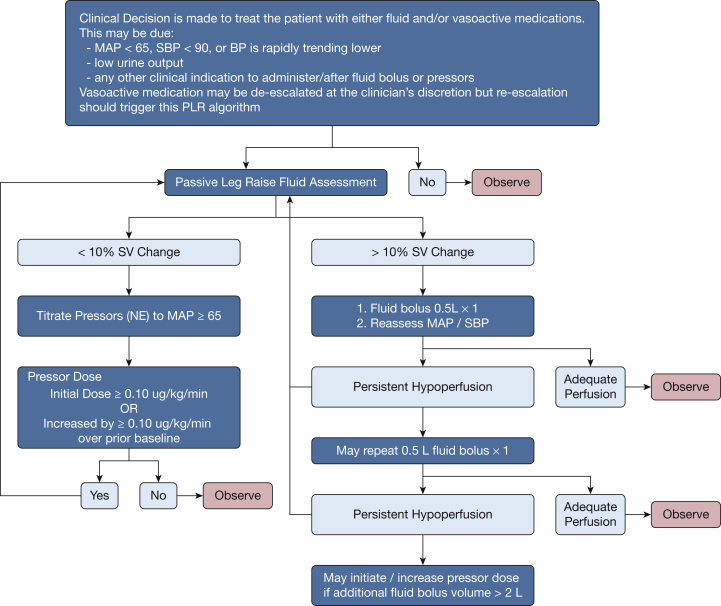
Study design and methods: We conducted a prospective, multicenter, randomized clinical trial at 13 hospitals in the United States and United Kingdom. Patients presented to EDs with sepsis that was associated hypotension and anticipated ICU admission. Intervention arm patients were assessed for fluid responsiveness before clinically driven fluid bolus or increase in vasopressors occurred. The protocol included reassessment and therapy as indicated by the passive leg raise result. The control arm received usual care. The primary clinical outcome was positive fluid balance at 72 hours or ICU discharge, whichever occurred first.
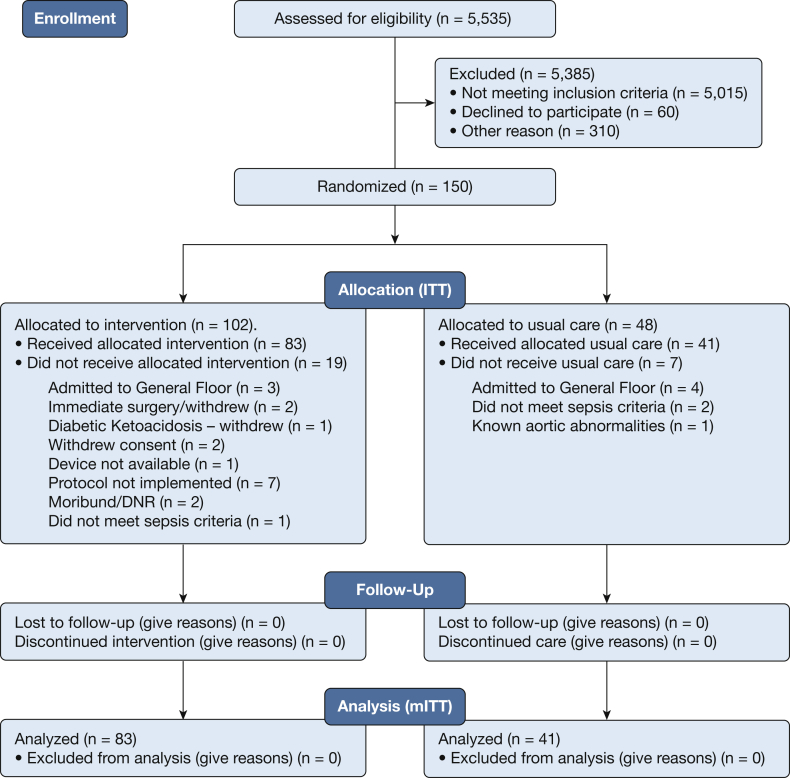
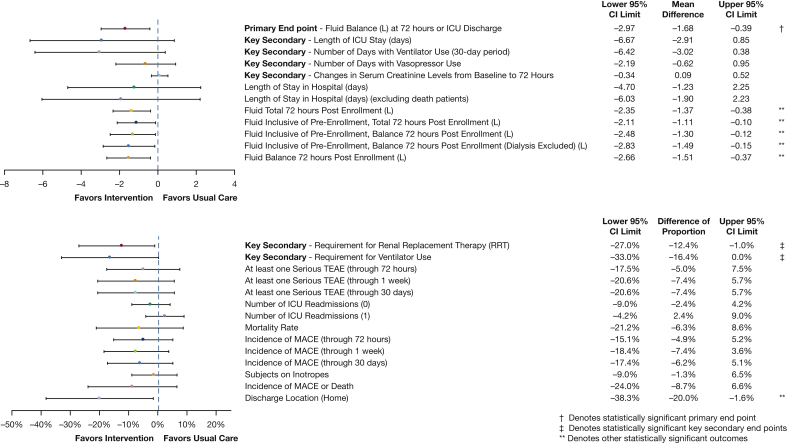
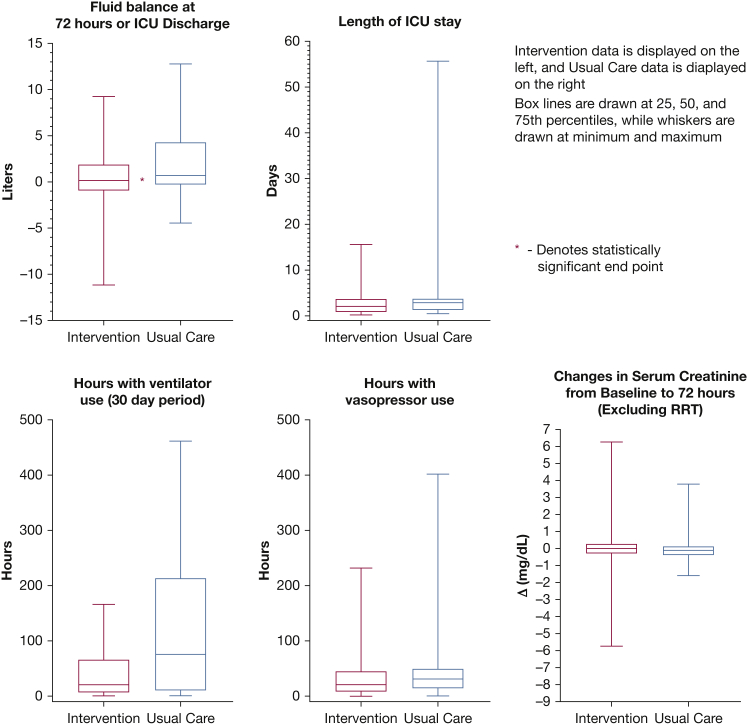
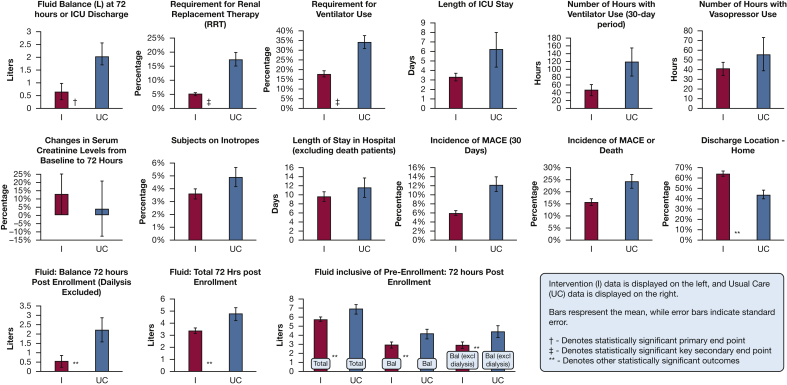
Results: In modified intent-to-treat analysis that included 83 intervention and 41 usual care eligible patients, fluid balance at 72 hours or ICU discharge was significantly lower (-1.37 L favoring the intervention arm; 0.65 ± 2.85 L intervention arm vs 2.02 ± 3.44 L usual care arm; P = .021. Fewer patients required renal replacement therapy (5.1% vs 17.5%; P = .04) or mechanical ventilation (17.7% vs 34.1%; P = .04) in the intervention arm compared with usual care. In the all-randomized intent-to-treat population (102 intervention, 48 usual care), there were no significant differences in safety signals.
Interpretation: Physiologically informed fluid and vasopressor resuscitation with the use of the passive leg raise-induced stroke volume change to guide management of septic shock is safe and demonstrated lower net fluid balance and reductions in the risk of renal and respiratory failure. Dynamic assessments to guide fluid administration may improve outcomes for patients with septic shock compared with usual care.
Clinical trial registration: NCT02837731.
Keywords: dynamic fluid response measure; hemodynamics; resuscitation; sepsis; shock.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Fluid Management in Sepsis Hypotension and Septic Shock: Time to Transition the Conversation From Fluid Responsive to Fluid Refractory?Chest. 2020 Oct;158(4):1319-1320. doi: 10.1016/j.chest.2020.05.524. Chest. 2020. PMID: 33036080 No abstract available.
-
The Impact of Management Using Fluid Response Evaluation on Renal and Respiratory Failure in Septic Shock.Chest. 2020 Dec;158(6):2706-2707. doi: 10.1016/j.chest.2020.06.088. Chest. 2020. PMID: 33280761 No abstract available.
-
Process Leading to Missing Data Has Meaning: Fluid Response Evaluation in Sepsis Hypotension and Shock.Chest. 2021 Mar;159(3):1300. doi: 10.1016/j.chest.2020.10.094. Chest. 2021. PMID: 33678254 No abstract available.
-
Fluid Responsiveness During Sepsis: The Unintended Intervention.Chest. 2021 Jul;160(1):e91-e92. doi: 10.1016/j.chest.2021.02.077. Chest. 2021. PMID: 34246403 Free PMC article. No abstract available.
References
-
- Levy M.M., Evans L.E., Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med. 2018;46(6):997–1000. - PubMed
-
- Brotfain E., Koyfman L., Toledano R., et al. Positive fluid balance as a major predictor of clinical outcome of patients with sepsis/septic shock after ICU discharge. Am J Emerg Med. 2016;34(11):2122–2126. - PubMed
-
- Wiedemann H.P., Wheeler A.P., Bernard G.R., et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564–2575. - PubMed
