

Renal, Cardiovascular, and Safety Outcomes of Canagliflozin by Baseline Kidney Function: A Secondary Analysis of the CREDENCE Randomized Trial
- PMID: 32354987
- PMCID: PMC7217416
- DOI: 10.1681/ASN.2019111168
Renal, Cardiovascular, and Safety Outcomes of Canagliflozin by Baseline Kidney Function: A Secondary Analysis of the CREDENCE Randomized Trial
Abstract
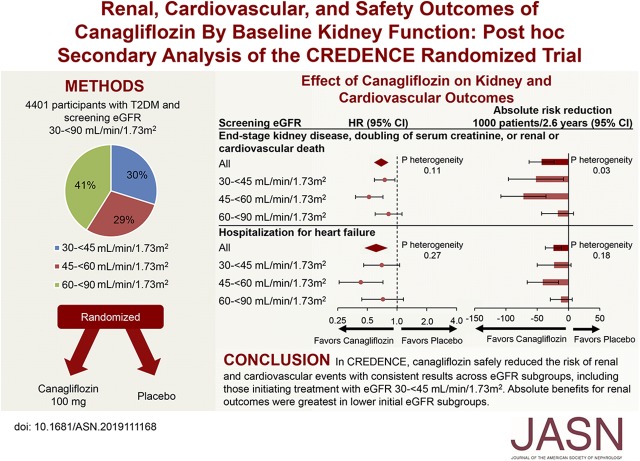
Background: Canagliflozin reduced renal and cardiovascular events in people with type 2 diabetes in the CREDENCE trial. We assessed efficacy and safety of canagliflozin by initial estimated glomerular filtration rate (eGFR).
Methods: CREDENCE randomly assigned 4401 participants with an eGFR of 30 to <90 ml/min per 1.73 m2 and substantial albuminuria to canagliflozin 100 mg or placebo. We used Cox proportional hazards regression to analyze effects on renal and cardiovascular efficacy and safety outcomes within screening eGFR subgroups (30 to <45, 45 to <60, and 60 to <90 ml/min per 1.73 m2) and linear mixed effects models to analyze the effects on eGFR slope.
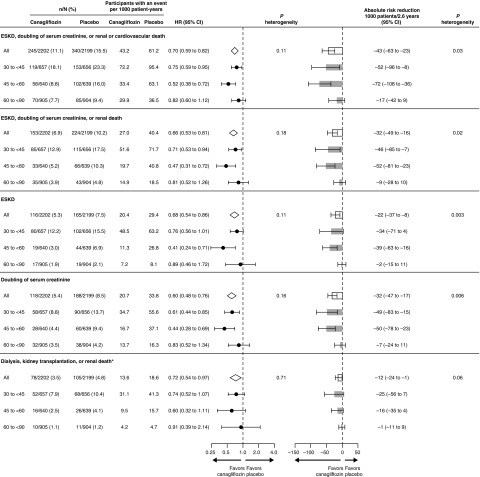
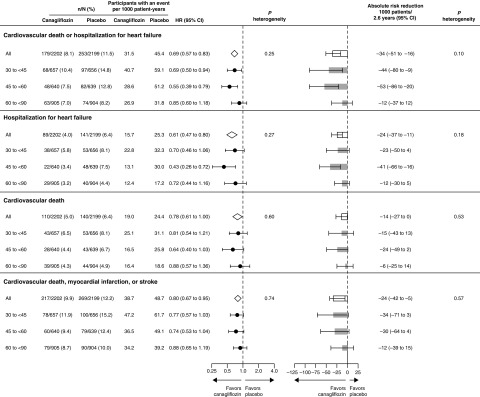
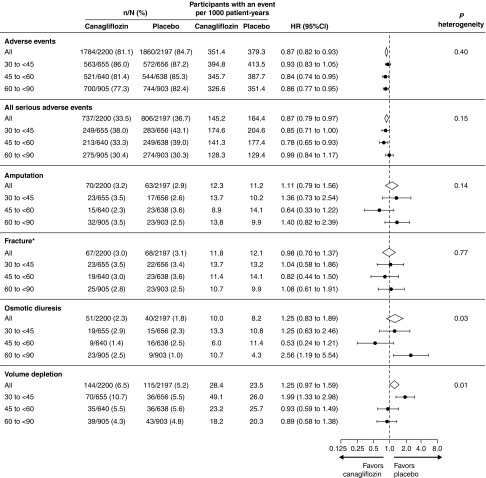
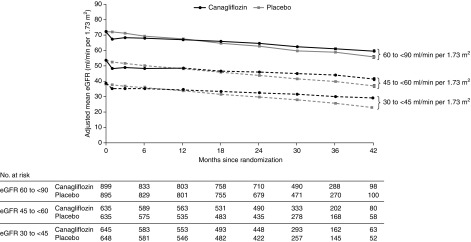
Results: At screening, 1313 (30%), 1279 (29%), and 1809 (41%) participants had an eGFR of 30 to <45, 45 to <60, and 60 to <90 ml/min per 1.73 m2, respectively. The relative benefits of canagliflozin for renal and cardiovascular outcomes appeared consistent among eGFR subgroups (all P interaction >0.11). Subgroups with lower eGFRs, who were at greater risk, exhibited larger absolute benefits for renal outcomes. Canagliflozin's lack of effect on serious adverse events, amputations, and fractures appeared consistent among eGFR subgroups. In all subgroups, canagliflozin use led to an acute eGFR drop followed by relative stabilization of eGFR loss. Among those with an eGFR of 30 to <45 ml/min per 1.73 m2, canagliflozin led to an initial drop of 2.03 ml/min per 1.73 m2. Thereafter, decline in eGFR was slower in the canagliflozin versus placebo group (-1.72 versus -4.33 ml/min per 1.73 m2; between-group difference 2.61 ml/min per 1.73 m2).
Conclusions: Canagliflozin safely reduced the risk of renal and cardiovascular events, with consistent results across eGFR subgroups, including the subgroup initiating treatment with an eGFR of 30 to <45 ml/min per 1.73 m2. Absolute benefits for renal outcomes were greatest in subgroups with lower eGFR.
Clinical trial registry name and registration number: Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy (CREDENCE), NCT02065791.
Keywords: SGLT2 inhibitor; canagliflozin; chronic kidney disease; diabetes; end-stage kidney disease.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Yamout H, Perkovic V, Davies M, Woo V, de Zeeuw D, Mayer C, et al.: Efficacy and safety of canagliflozin in patients with type 2 diabetes and stage 3 nephropathy. Am J Nephrol 40: 64–74, 2014 - PubMed
-
- INVOKANA (canagliflozin) tablets, for oral use [package insert]. Titusville, NJ, Janssen Pharmaceuticals, 2013.
-
- FARXIGA (dapagliflozin) tablets, for oral use [package insert]. Princeton, NJ, Bristol-Myers Squibb Company, 2014.
-
- JARDIANCE (empagliflozin) tablets, for oral use [package insert]. Ridgefield, CT, Boehringer Ingelheim Pharmaceuticals, 2014.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
