

J-CKD-DB: a nationwide multicentre electronic health record-based chronic kidney disease database in Japan
- PMID: 32355258
- PMCID: PMC7192920
- DOI: 10.1038/s41598-020-64123-z
J-CKD-DB: a nationwide multicentre electronic health record-based chronic kidney disease database in Japan
Abstract
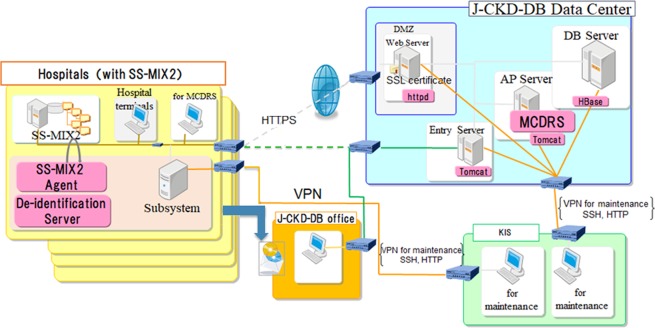
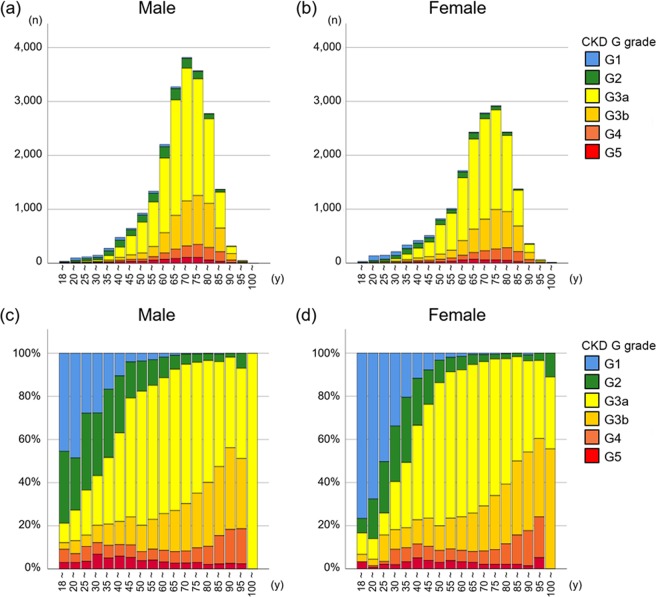
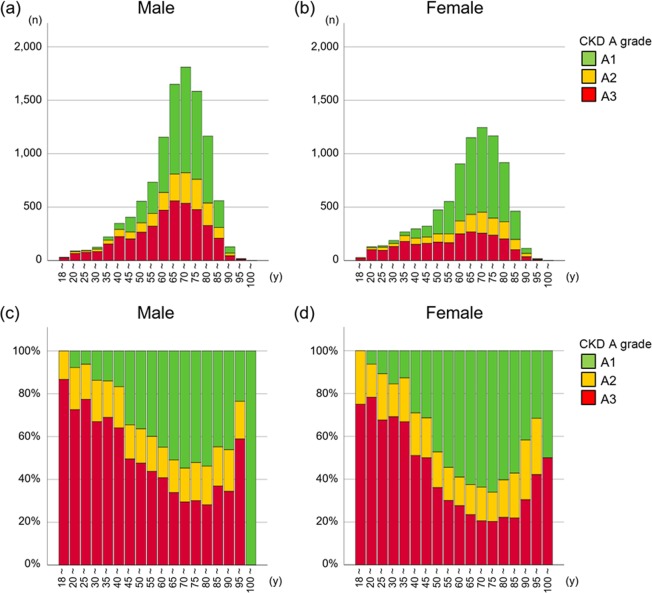
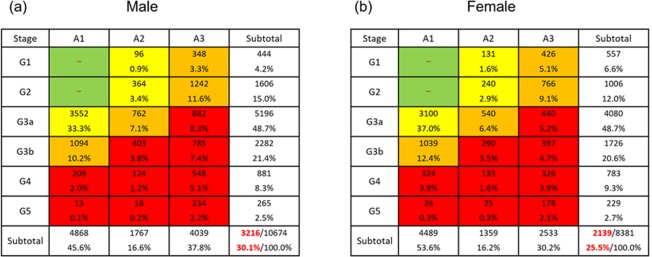
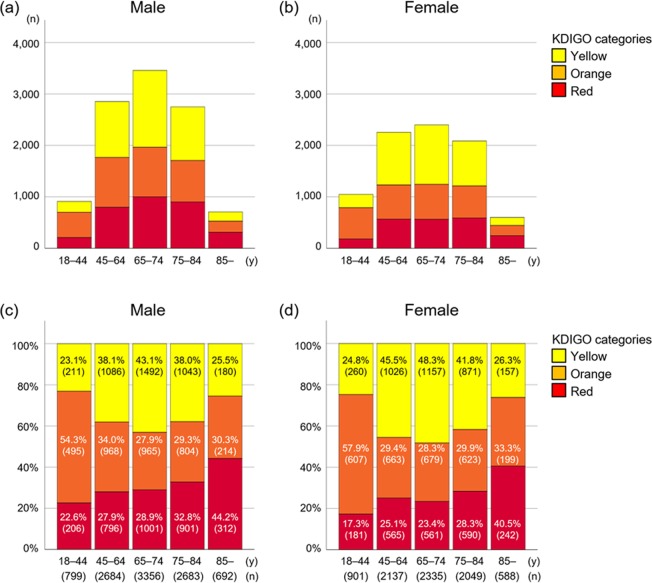
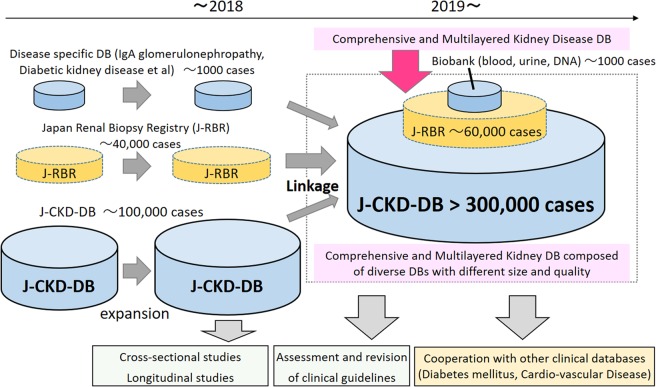
The Japan Chronic Kidney Disease (CKD) Database (J-CKD-DB) is a large-scale, nation-wide registry based on electronic health record (EHR) data from participating university hospitals. Using a standardized exchangeable information storage, the J-CKD-DB succeeded to efficiently collect clinical data of CKD patients across hospitals despite their different EHR systems. CKD was defined as dipstick proteinuria ≥1+ and/or estimated glomerular filtration rate <60 mL/min/1.73 m2 base on both out- and inpatient laboratory data. As an initial analysis, we analyzed 39,121 CKD outpatients (median age was 71 years, 54.7% were men, median eGFR was 51.3 mL/min/1.73 m2) and observed that the number of patients with a CKD stage G1, G2, G3a, G3b, G4 and G5 were 1,001 (2.6%), 2,612 (6.7%), 23,333 (59.6%), 8,357 (21.4%), 2,710 (6.9%) and 1,108 (2.8%), respectively. According to the KDIGO risk classification, there were 30.1% and 25.5% of male and female patients with CKD at very high-risk, respectively. As the information from every clinical encounter from those participating hospitals will be continuously updated with an anonymized patient ID, the J-CKD-DB will be a dynamic registry of Japanese CKD patients by expanding and linking with other existing databases and a platform for a number of cross-sectional and prospective analyses to answer important clinical questions in CKD care.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
