

Instability and excessive mechanical loading mediate subchondral bone changes to induce osteoarthritis
- PMID: 32355794
- PMCID: PMC7186756
- DOI: 10.21037/atm.2020.02.103
Instability and excessive mechanical loading mediate subchondral bone changes to induce osteoarthritis
Abstract
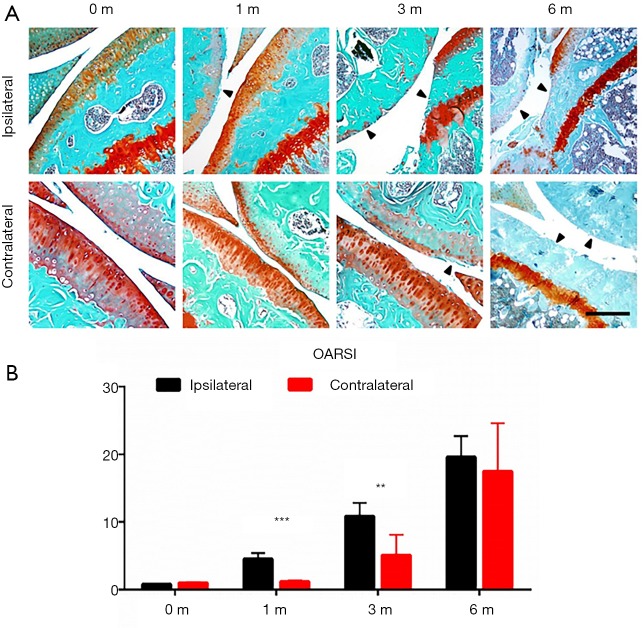
Background: To assess the diversified effects of mechanical instability, excessive mechanical loading on subchondral bone remodeling. And to investigate the underlying cartilage degeneration and osteoarthritis (OA) progression in ipsilateral and contralateral knees, given that OA progression always affects joints bilaterally.
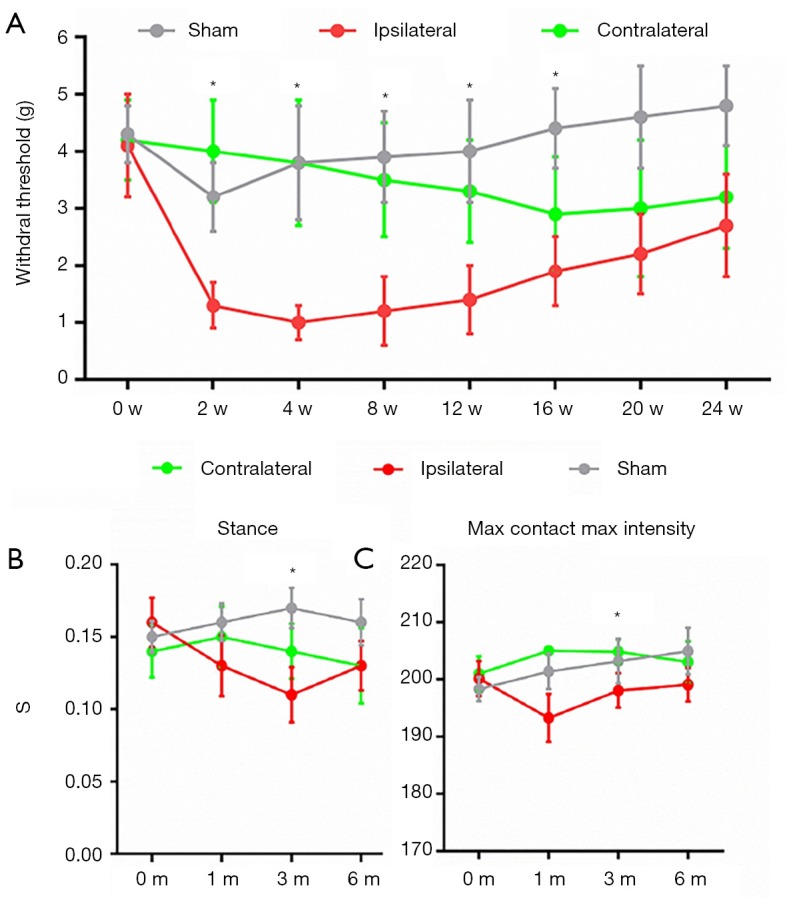
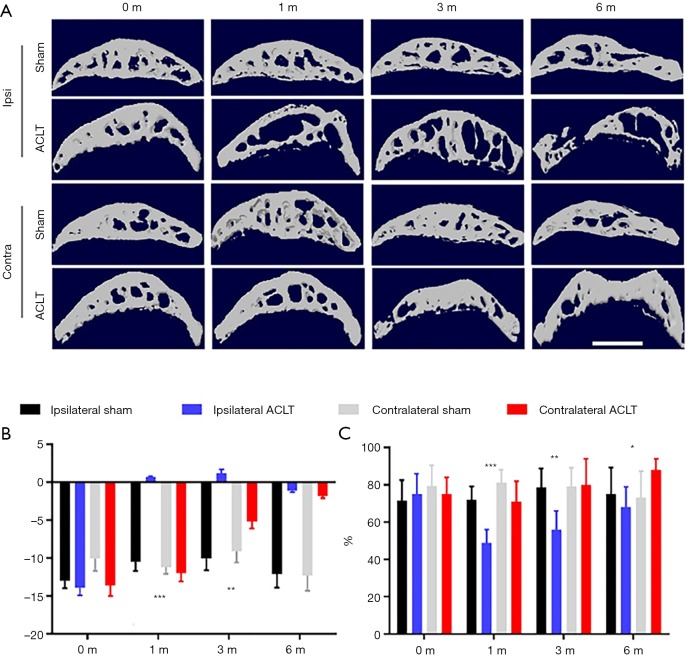
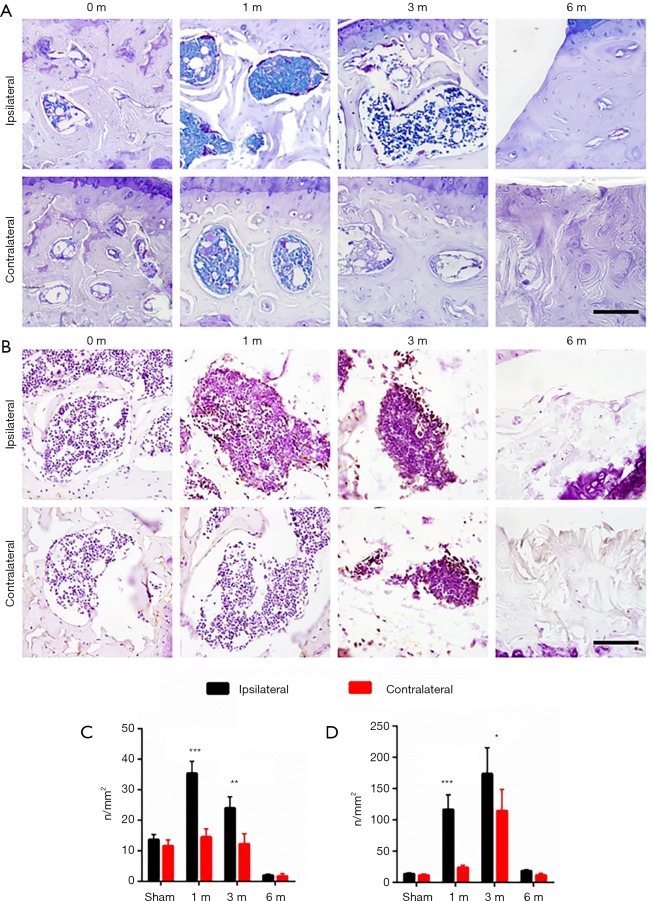
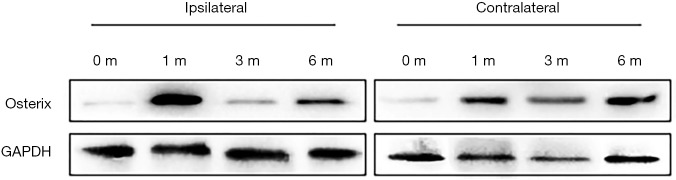
Methods: Anterior cruciate ligament transection (ACLT) of the left knee was used to induce OA in C57/B6 mice for 1, 3 and 6 months. Both left (ipsilateral) and right (contralateral) knees underwent micro-computerized tomography (micro-CT) scan and morphological analysis. The subchondral bone metabolism analysis by immunostaining of tartrate-resistant acid phosphatase (TRAP) and Osterix. Behavioral analyses including von Frey test and CatWalk gait analysis were also performed. Western blot analysis was performed to assess the signaling pathways involved in OA progression.
Results: Analyses showed that various changes in ipsilateral and contralateral knees lead to OA progression. Articular cartilage was rapidly destroyed on the ipsilateral side but was only gradually destroyed on the contralateral side. Micro-CT data showed a rapid decrease with a subsequent partial recovery of bone volume in the late stage on the ipsilateral side, while a gradual condensation of bone density was seen on the contralateral side. Immunostaining showed increased osteoclastic and osteoblastic activity in the early stage on the ipsilateral side, but only slight osteoblastic changes on the contralateral side. Behavioral analyses including von Frey and gait analysis showed that contralateral knees compensate ipsilateral mechanical loading, but also that this mechanism failed to work in the late stage.
Conclusions: Diversified mechanical loading properties lead to OA progression through different mechanisms of subchondral bone remodeling. Acute ACLT led to OA through bone density reduction, while the contralateral side developed OA gradually due to subchondral bone sclerosis.
Keywords: Osteoarthritis (OA); contralateral side; mechanical loading; subchondral bone.
2020 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: YL serves as an unpaid section editor of Annals of Translational Medicine from Oct 2019 to Sep 2020. The other authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources