

Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19
- PMID: 32356626
- PMCID: PMC7206931
- DOI: 10.1056/NEJMoa2007621
Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19
Retraction in
-
Retraction: Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19. N Engl J Med. DOI: 10.1056/NEJMoa2007621.N Engl J Med. 2020 Jun 25;382(26):2582. doi: 10.1056/NEJMc2021225. Epub 2020 Jun 4. N Engl J Med. 2020. PMID: 32501665 Free PMC article. No abstract available.
Expression of concern in
-
Expression of Concern: Mehra MR et al. Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19. N Engl J Med. DOI: 10.1056/NEJMoa2007621.N Engl J Med. 2020 Jun 18;382(25):2464. doi: 10.1056/NEJMe2020822. Epub 2020 Jun 2. N Engl J Med. 2020. PMID: 32484612 Free PMC article. No abstract available.
Abstract
Background: Coronavirus disease 2019 (Covid-19) may disproportionately affect people with cardiovascular disease. Concern has been aroused regarding a potential harmful effect of angiotensin-converting-enzyme (ACE) inhibitors and angiotensin-receptor blockers (ARBs) in this clinical context.
Methods: Using an observational database from 169 hospitals in Asia, Europe, and North America, we evaluated the relationship of cardiovascular disease and drug therapy with in-hospital death among hospitalized patients with Covid-19 who were admitted between December 20, 2019, and March 15, 2020, and were recorded in the Surgical Outcomes Collaborative registry as having either died in the hospital or survived to discharge as of March 28, 2020.
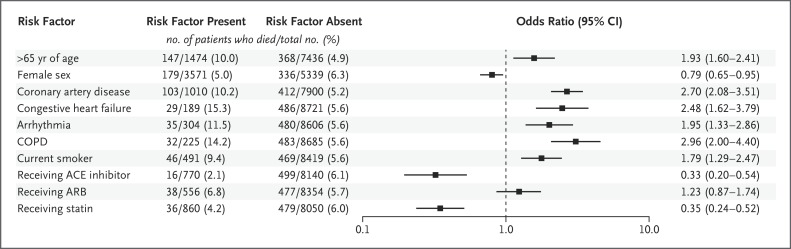
Results: Of the 8910 patients with Covid-19 for whom discharge status was available at the time of the analysis, a total of 515 died in the hospital (5.8%) and 8395 survived to discharge. The factors we found to be independently associated with an increased risk of in-hospital death were an age greater than 65 years (mortality of 10.0%, vs. 4.9% among those ≤65 years of age; odds ratio, 1.93; 95% confidence interval [CI], 1.60 to 2.41), coronary artery disease (10.2%, vs. 5.2% among those without disease; odds ratio, 2.70; 95% CI, 2.08 to 3.51), heart failure (15.3%, vs. 5.6% among those without heart failure; odds ratio, 2.48; 95% CI, 1.62 to 3.79), cardiac arrhythmia (11.5%, vs. 5.6% among those without arrhythmia; odds ratio, 1.95; 95% CI, 1.33 to 2.86), chronic obstructive pulmonary disease (14.2%, vs. 5.6% among those without disease; odds ratio, 2.96; 95% CI, 2.00 to 4.40), and current smoking (9.4%, vs. 5.6% among former smokers or nonsmokers; odds ratio, 1.79; 95% CI, 1.29 to 2.47). No increased risk of in-hospital death was found to be associated with the use of ACE inhibitors (2.1% vs. 6.1%; odds ratio, 0.33; 95% CI, 0.20 to 0.54) or the use of ARBs (6.8% vs. 5.7%; odds ratio, 1.23; 95% CI, 0.87 to 1.74).
Conclusions: Our study confirmed previous observations suggesting that underlying cardiovascular disease is associated with an increased risk of in-hospital death among patients hospitalized with Covid-19. Our results did not confirm previous concerns regarding a potential harmful association of ACE inhibitors or ARBs with in-hospital death in this clinical context. (Funded by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women's Hospital.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Mortality in COVID-19 patients treated with ACEIs/ARBs: Re-estimated meta-analysis results following the Mehra et al. retraction.Pharmacol Res. 2020 Oct;160:105053. doi: 10.1016/j.phrs.2020.105053. Epub 2020 Jun 30. Pharmacol Res. 2020. PMID: 32619721 Free PMC article. Retracted. No abstract available.
-
Meeting the Challenge of Scientific Dissemination in the Era of COVID-19: Toward a Modular Approach to Knowledge-Sharing for Radiation Oncology.Int J Radiat Oncol Biol Phys. 2020 Oct 1;108(2):496-505. doi: 10.1016/j.ijrobp.2020.06.066. Int J Radiat Oncol Biol Phys. 2020. PMID: 32890543 Free PMC article. No abstract available.
References
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous