

Diagnostic accuracy of a novel tuberculosis point-of-care urine lipoarabinomannan assay for people living with HIV: A meta-analysis of individual in- and outpatient data
- PMID: 32357197
- PMCID: PMC7194366
- DOI: 10.1371/journal.pmed.1003113
Diagnostic accuracy of a novel tuberculosis point-of-care urine lipoarabinomannan assay for people living with HIV: A meta-analysis of individual in- and outpatient data
Abstract
Background: Tuberculosis (TB) is the most common cause of death in people living with HIV (PLHIV), yet TB often goes undiagnosed since many patients are not able to produce a sputum specimen, and traditional diagnostics are costly or unavailable. A novel, rapid lateral flow assay, Fujifilm SILVAMP TB LAM (SILVAMP-LAM), detects the presence of TB lipoarabinomannan (LAM) in urine, and is substantially more sensitive for diagnosing TB in PLHIV than an earlier LAM assay (Alere Determine TB LAM lateral flow assay [LF-LAM]). Here, we present an individual participant data meta-analysis of the diagnostic accuracy of SILVAMP-LAM in adult PLHIV, including both published and unpublished data.
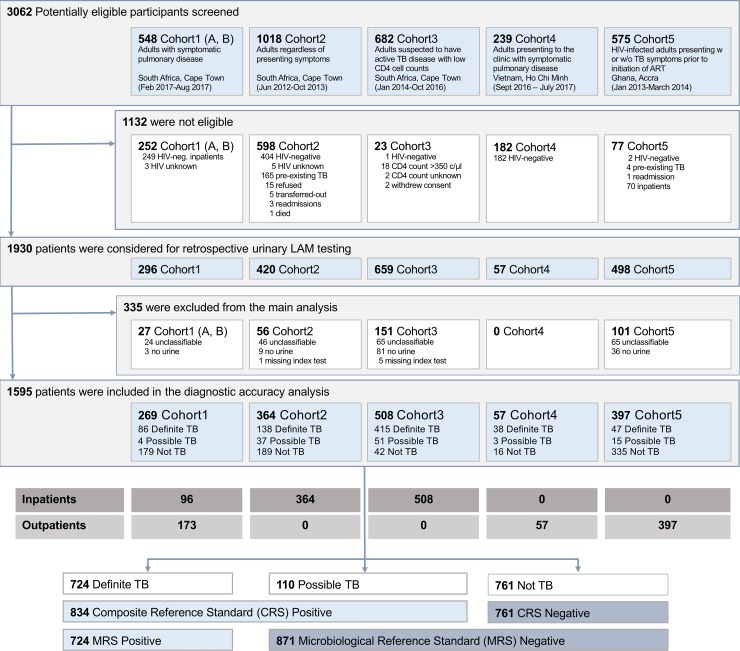
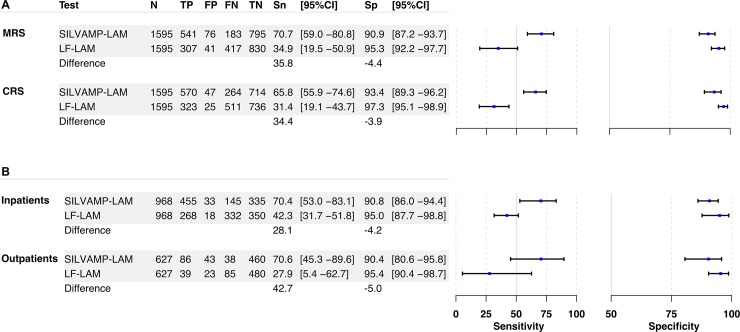
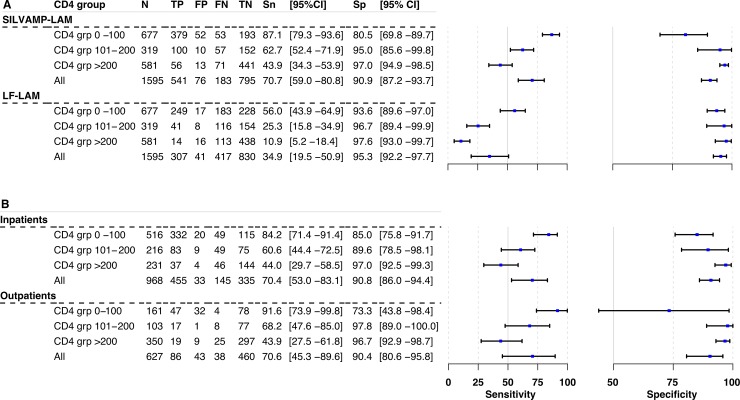
Methods and findings: Adult PLHIV (≥18 years) were assessed in 5 prospective cohort studies in South Africa (3 cohorts), Vietnam, and Ghana, carried out during 2012 to 2017. Of the 1,595 PLHIV who met eligibility criteria, the majority (61%) were inpatients, median age was 37 years (IQR 30-43), 43% had a CD4 count ≤ 100 cells/μl, and 35% were receiving antiretroviral therapy. Most participants (94%) had a positive WHO symptom screen for TB on enrollment, and 45% were diagnosed with microbiologically confirmed TB, using mycobacterial culture or Xpert MTB/RIF testing of sputum, urine, or blood. Previously published data from inpatients were combined with unpublished data from outpatients. Biobanked urine samples were tested, using blinded double reading, with SILVAMP-LAM and LF-LAM. Applying a microbiological reference standard for assessment of sensitivity, the overall sensitivity for TB detection was 70.7% (95% CI 59.0%-80.8%) for SILVAMP-LAM compared to 34.9% (95% CI 19.5%-50.9%) for LF-LAM. Using a composite reference standard (which included patients with both microbiologically confirmed as well as clinically diagnosed TB), SILVAMP-LAM sensitivity was 65.8% (95% CI 55.9%-74.6%), and that of LF-LAM 31.4% (95% CI 19.1%-43.7%). In patients with CD4 count ≤ 100 cells/μl, SILVAMP-LAM sensitivity was 87.1% (95% CI 79.3%-93.6%), compared to 56.0% (95% CI 43.9%-64.9%) for LF-LAM. In patients with CD4 count 101-200 cells/μl, SILVAMP-LAM sensitivity was 62.7% (95% CI 52.4%-71.9%), compared to 25.3% (95% CI 15.8%-34.9%) for LF-LAM. In those with CD4 count > 200 cells/μl, SILVAMP-LAM sensitivity was 43.9% (95% CI 34.3%-53.9%), compared to 10.9% (95% CI 5.2%-18.4%) for LF-LAM. Using a microbiological reference standard, the specificity of SILVAMP-LAM was 90.9% (95% CI 87.2%-93.7%), and that of LF-LAM 95.3% (95% CI 92.2%-97.7%). Limitations of this study include the use of biobanked, rather than fresh urine samples, and testing by skilled laboratory technicians in research laboratories, rather than at the point of care.
Conclusions: In this study, we found that SILVAMP-LAM identified a substantially higher proportion of TB patients in PLHIV than LF-LAM. The sensitivity of SILVAMP-LAM was highest in patients with CD4 count ≤ 100 cells/μl. Further work is needed to demonstrate accuracy when implemented as a point-of-care test.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: TB, SGS, AM, SO, RS and CMD were previously or are currently employed by FIND. TB reports a patent in the field of lipoarabinomannan detection. CMD is a member of PLOS Medicine's Editorial Board. The rest of the authors declare no competing interests associated with this manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Figures
References
-
- Gupta-Wright A, Corbett EL, van Oosterhout JJ, Wilson D, Grint D, Alufandika-Moyo M, et al. Rapid urine-based screening for tuberculosis in HIV-positive patients admitted to hospital in Africa (STAMP): a pragmatic, multicentre, parallel-group, double-blind, randomised controlled trial. Lancet. 2018;392:292–301. 10.1016/S0140-6736(18)31267-4 - DOI - PMC - PubMed
-
- Peter JG, Zijenah LS, Chanda D, Clowes P, Lesosky M, Gina P, et al. Effect on mortality of point-of-care, urine-based lipoarabinomannan testing to guide tuberculosis treatment initiation in HIV-positive hospital inpatients: a pragmatic, parallel-group, multicountry, open-label, randomised controlled trial. Lancet. 2016;387:1187–97. 10.1016/S0140-6736(15)01092-2 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
