

Intramedullary cervical spinal cord teratoma
- PMID: 32358400
- PMCID: PMC7440273
- DOI: 10.1097/MD.0000000000020107
Intramedullary cervical spinal cord teratoma
Abstract
Background: Intramedullary cervical spinal cord teratomas (ICTs) are extremely rare, and diagnosis and treatment are challenging. We conducted a systematic review of the literature on the diagnosis and treatment of ICT.
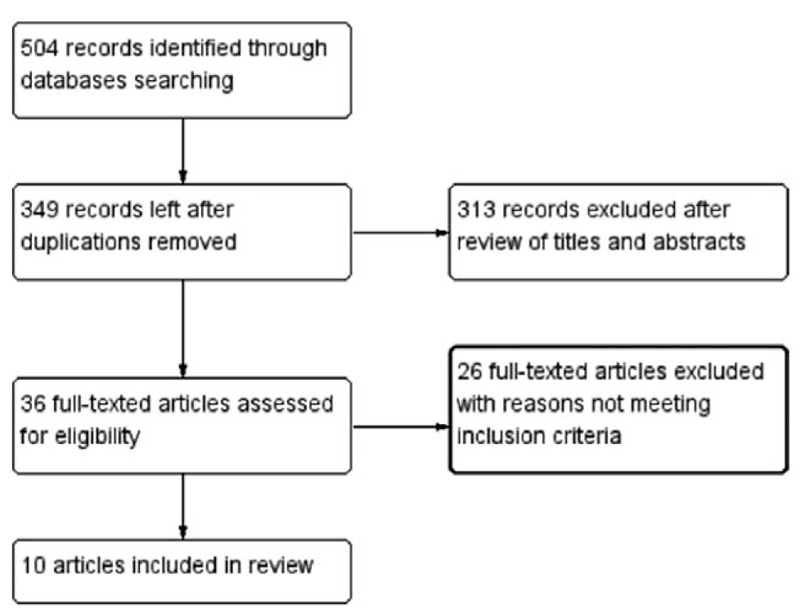
Method: The presentation, imaging manifestations, diagnosis, management, surgery findings, prognosis and histology were reviewed following Preferred Reporting Items for Systematic Reviews and Meta Analyses guidelines. English-language studies and case reports published from inception to 2018 were retrieved. Data on presentation, imaging characteristics, diagnosis, management, surgery findings, outcomes, and histopathology were extracted.
Results: Ten articles involving 10 patients were selected. The lesions were located in the upper cervical vertebrae in 4 cases, whereas in the lower cervical vertebrae in the remaining 6 cases. In 5 cases, the lesions were located on the dorsal side of the spinal cord, and in the center of the spinal cord in the remaining 5 cases. Quadriparesis (60%), paraplegia (30%), monoplegia (10%), and neck pain (50%) were the main presentations. The lesion appeared as a intramedullary heterogeneous signal during an MRI scan, and the lesion signal would be partially enhanced after the contrast medium was applied. All patients underwent surgical intervention through a posterior approach. Neurological function improved postoperatively in all patients. Two patients with pathology confirmed to be immature teratomas experienced recurrence.
Conclusion: ICTs are extremely rare entities that are mainly located in the center or dorsal part of the spinal cord which mainly manifest as quadriplegia and neck pain. MRI is a useful modality that provides diagnostic clues. Surgery from a posterior approach is the primary treatment, and the effect of adjuvant therapy remains uncertain. The prognosis is mainly related to the pathological nature of the tumor and not the method of resection.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures


References
-
- Turan N, Halani SH, Baum GR, et al. Adult intramedullary teratoma of the spinal cord: a case report and review of literature. World Neurosurg 2016;87: 661.e23–661.e6.61E30. - PubMed
-
- Mohammadi A, Fereydouni T, Rahbari A, et al. Intradural intramedullary teratoma presenting in the lumbar spine: report of a rare case. World Neurosurg 2017;106: 1051.e5–1051.e8. - PubMed
-
- Nickols HH, Chambless LB, Carson RP, et al. Intramedullary spinal immature teratoma: resolution of quadriplegia following resection in a 4-week-old infant. J Neurosurg Pediatr 2010;6:586–91. - PubMed
-
- Tsitsopoulos P, Rizos C, Isaakidis D, et al. Coexistence of spinal intramedullary teratoma and diastematomyelia in an adult. Spinal Cord 2006;44:632–5. - PubMed
-
- Poeze M, Herpers MJ, Tjandra B, et al. Intramedullary spinal teratoma presenting with urinary retention: case report and review of the literature. Neurosurgery 1999;45:379–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
