

The first, holistic immunological model of COVID-19: Implications for prevention, diagnosis, and public health measures
- PMID: 32359201
- PMCID: PMC7267459
- DOI: 10.1111/pai.13271
The first, holistic immunological model of COVID-19: Implications for prevention, diagnosis, and public health measures
Abstract
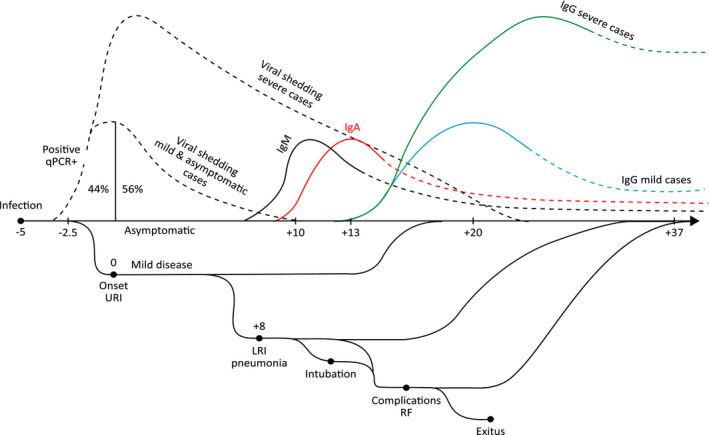
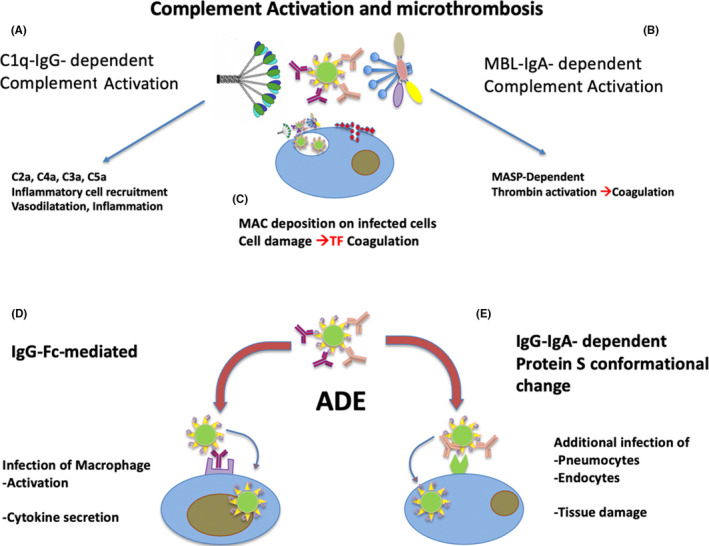
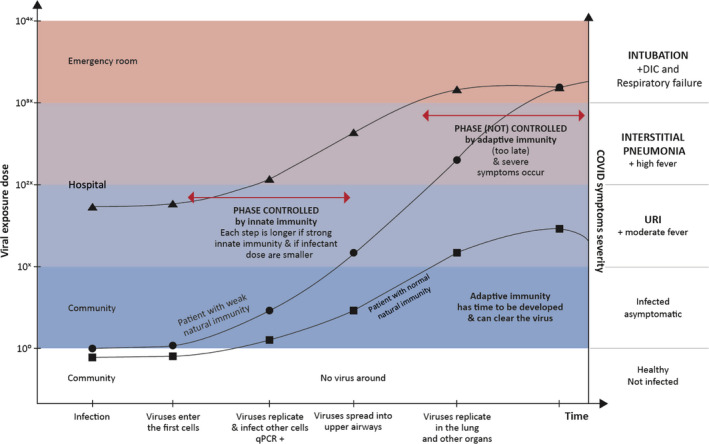
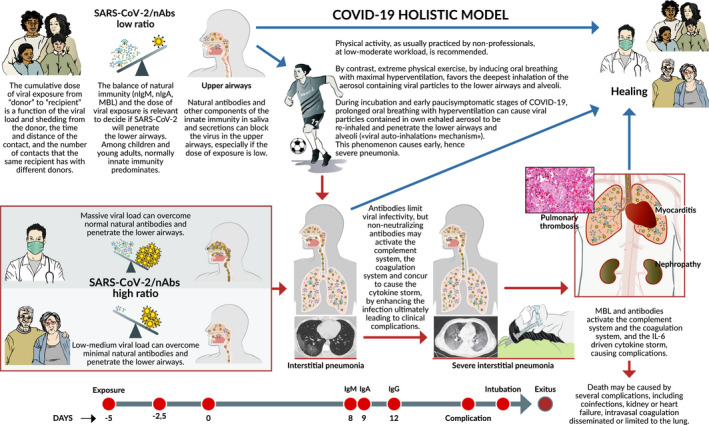
The natural history of COVID-19 caused by SARS-CoV-2 is extremely variable, ranging from asymptomatic or mild infection, mainly in children, to multi-organ failure, eventually fatal, mainly in the eldest. We propose here the first model explaining how the outcome of first, crucial 10-15 days after infection, depends on the balance between the cumulative dose of viral exposure and the efficacy of the local innate immune response (natural IgA and IgM antibodies, mannose-binding lectin). If SARS-CoV-2 runs the blockade of this innate immunity and spreads from the upper airways to the alveoli in the early phases of the infections, it can replicate with no local resistance, causing pneumonia and releasing high amounts of antigens. The delayed and strong adaptive immune response (high-affinity IgM and IgG antibodies) that follows, causes severe inflammation and triggers mediator cascades (complement, coagulation, and cytokine storm), leading to complications often requiring intensive therapy and being, in some patients, fatal. Low-moderate physical activity can still be recommended. However, extreme physical activity and oral breathing with hyperventilation during the incubation days and early stages of COVID-19 facilitates re-inhalation and early direct penetration of high numbers of own virus particles in the lower airways and the alveoli, without impacting on the airway's mucosae covered by neutralizing antibodies ("viral auto-inhalation" phenomenon). This allows the virus to bypass the efficient immune barrier of the upper airway mucosa in already infected, young, and otherwise healthy athletes. In conclusion, whether the virus or the adaptive immune response reaches the lungs first is a crucial factor deciding the fate of the patient. This "quantitative and time-/sequence-dependent" model has several implications for prevention, diagnosis, and therapy of COVID-19 at all ages.
Keywords: COVID-19; SARS-CoV-2; antibodies; glycans; immunoglobulin M; pneumonia; prediction; protection.
© 2020 The Authors. Pediatric Allergy and Immunology published by John Wiley & Sons Ltd.
Conflict of interest statement
The text contains the personal opinion of the Authors, not of their institutions: Charité Universitaetsmedizin Berlin, Germany (PMM), and Istituto Superiore di Sanità, Rome, Italy (RN). All authors declare no conflict of interest.
Figures
Comment in
-
Comment on Matricardi PM et al.Pediatr Allergy Immunol. 2020 Nov;31(8):997. doi: 10.1111/pai.13277. Epub 2020 Jun 12. Pediatr Allergy Immunol. 2020. PMID: 32418306 Free PMC article. No abstract available.
References
-
- Drosten C, Günther S, Preiser W, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967‐1976. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
