

Immunity and Hypertension
- PMID: 32359222
- PMCID: PMC7606441
- DOI: 10.1111/apha.13487
Immunity and Hypertension
Abstract
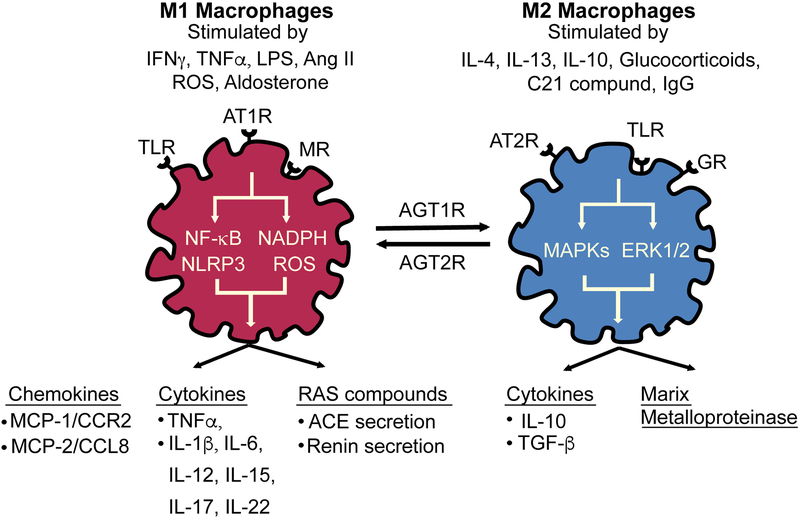
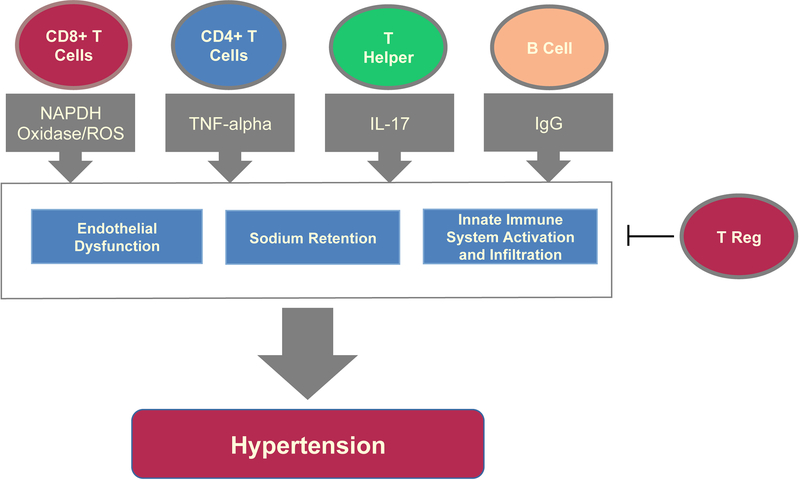
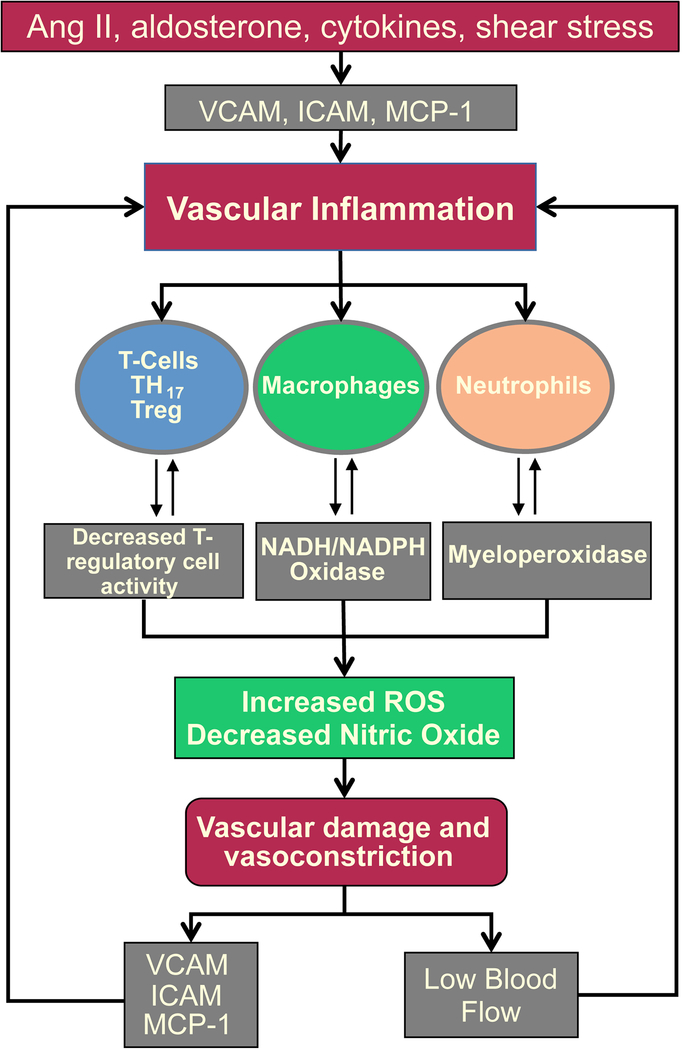
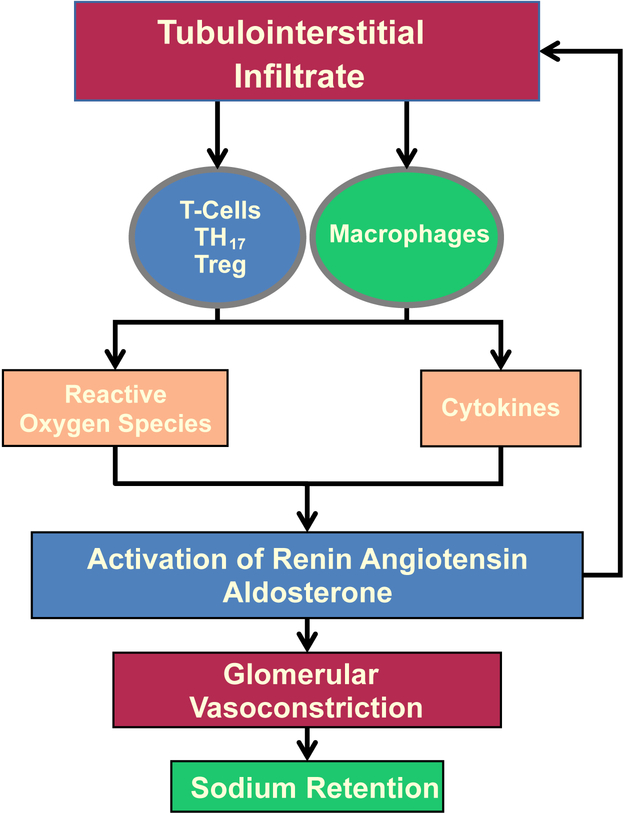
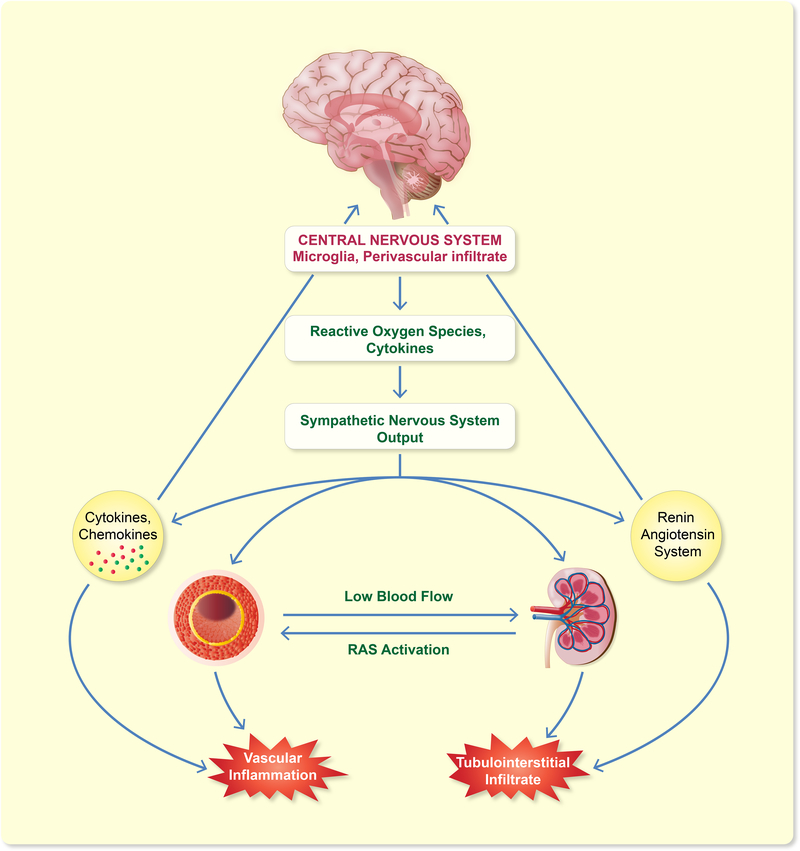
Hypertension is the primary cause of cardiovascular mortality. Despite multiple existing treatments, only half of those with the disease achieve adequate control. Therefore, understanding the mechanisms causing hypertension is essential for the development of novel therapies. Many studies demonstrate that immune cell infiltration of the vessel wall, kidney and central nervous system, as well as their counterparts of oxidative stress, the renal renin-angiotensin system (RAS) and sympathetic tone play a critical role in the development of hypertension. Genetically modified mice lacking components of innate and/or adaptive immunity confirm the importance of chronic inflammation in hypertension and its complications. Depletion of immune cells improves endothelial function, decreases oxidative stress, reduces vascular tone and prevents renal interstitial infiltrates, sodium retention and kidney damage. Moreover, the ablation of microglia or central nervous system perivascular macrophages reduces RAS-induced inflammation and prevents sympathetic nervous system activation and hypertension. Therefore, understanding immune cell functioning and their interactions with tissues that regulate hypertensive responses may be the future of novel antihypertensive therapies.
Keywords: Immunity; hypertension; lymphocytes; macrophages; reactive oxygen species; renin-angiotensin system.
© 2020 Scandinavian Physiological Society. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS data brief. 2013(133):1–8. - PubMed
-
- Svendsen UG. Evidence for an initial, thymus independent and a chronic, thymus dependent phase of DOCA and salt hypertension in mice. Acta Pathol Microbiol Scand A. 1976;84(6):523–528. - PubMed
-
- White FN, Grollman A. Autoimmune Factors Associated with Infarction of the Kidney. Nephron. 1964;1:93–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
