

Early Endothelial Dysfunction in Type 1 Diabetes Is Accompanied by an Impairment of Vascular Smooth Muscle Function: A Meta-Analysis
- PMID: 32362871
- PMCID: PMC7180178
- DOI: 10.3389/fendo.2020.00203
Early Endothelial Dysfunction in Type 1 Diabetes Is Accompanied by an Impairment of Vascular Smooth Muscle Function: A Meta-Analysis
Abstract
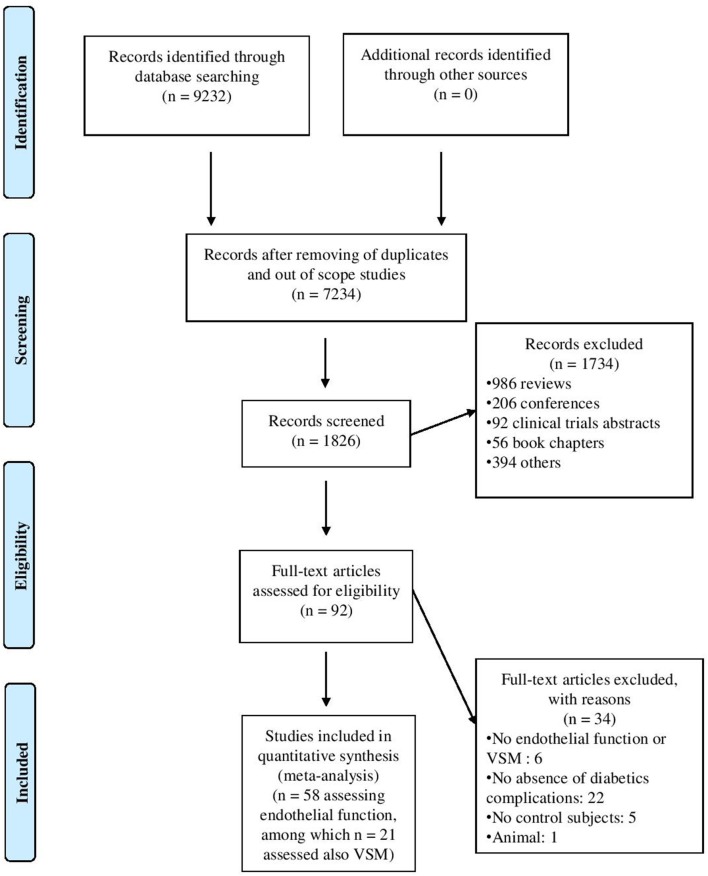
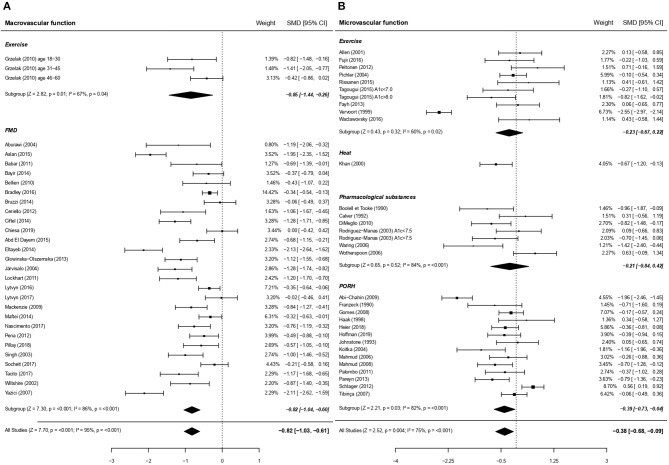
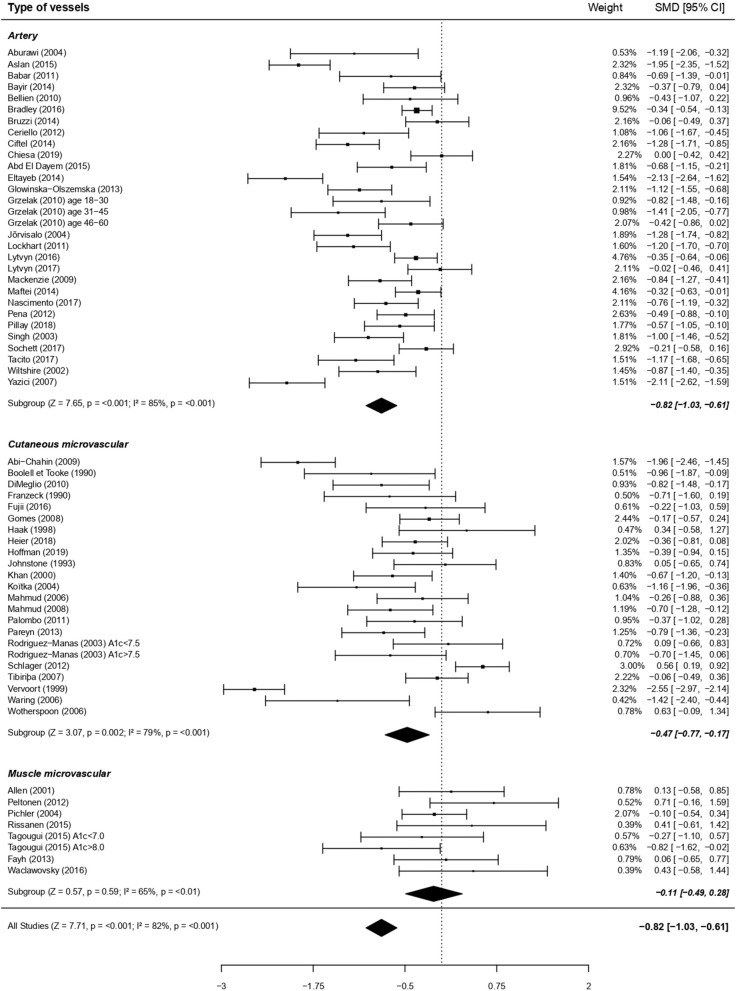
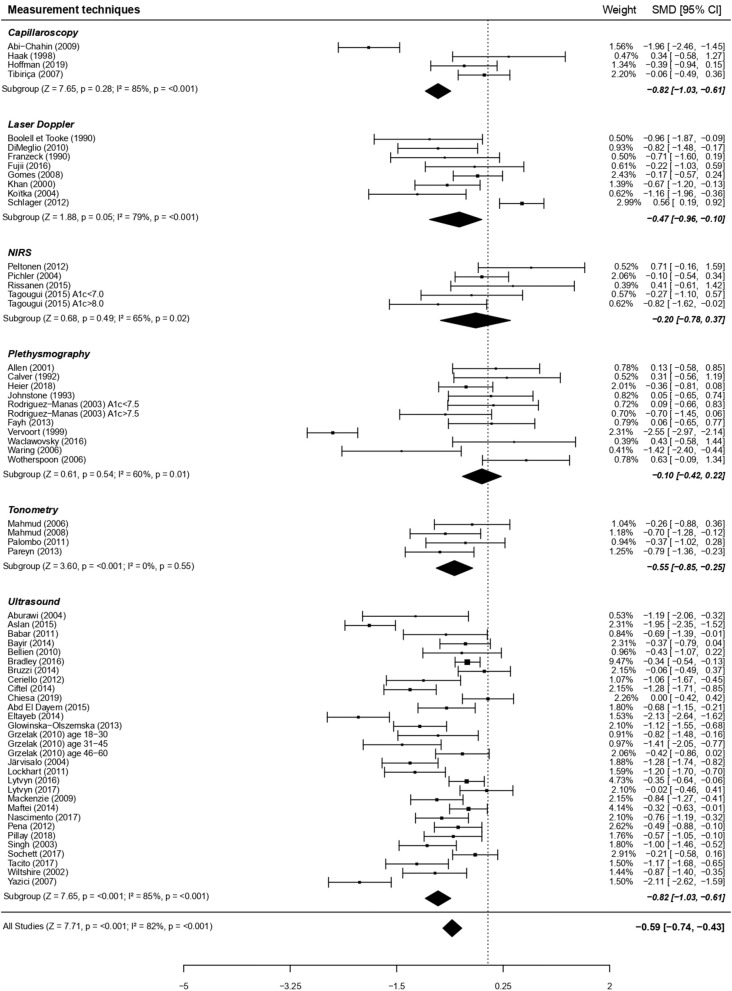
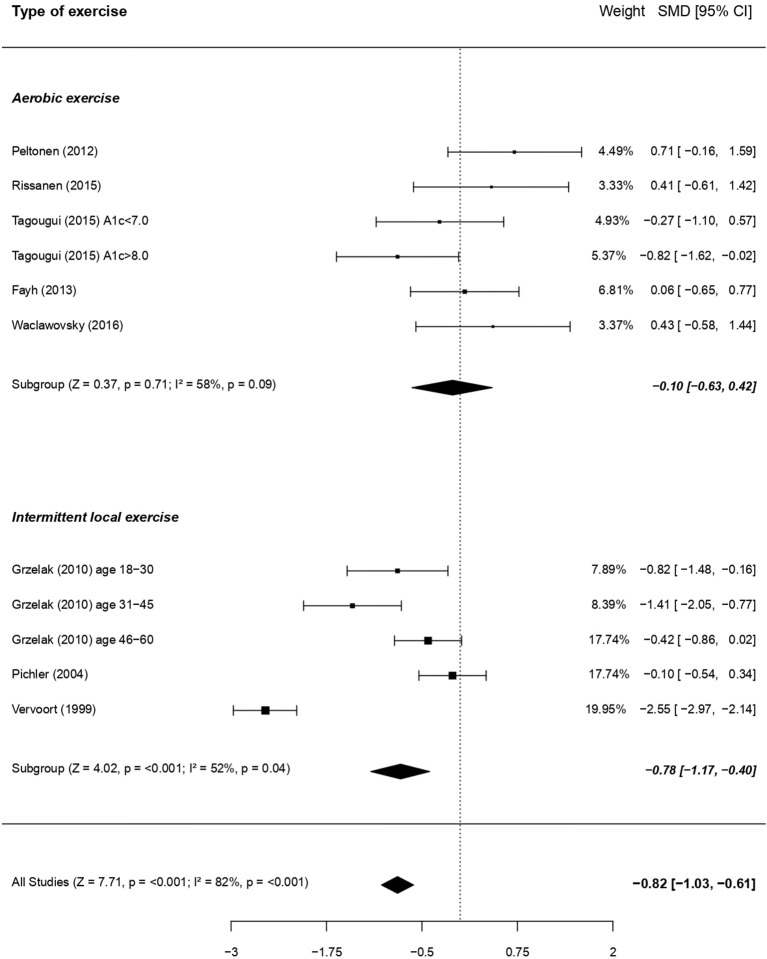
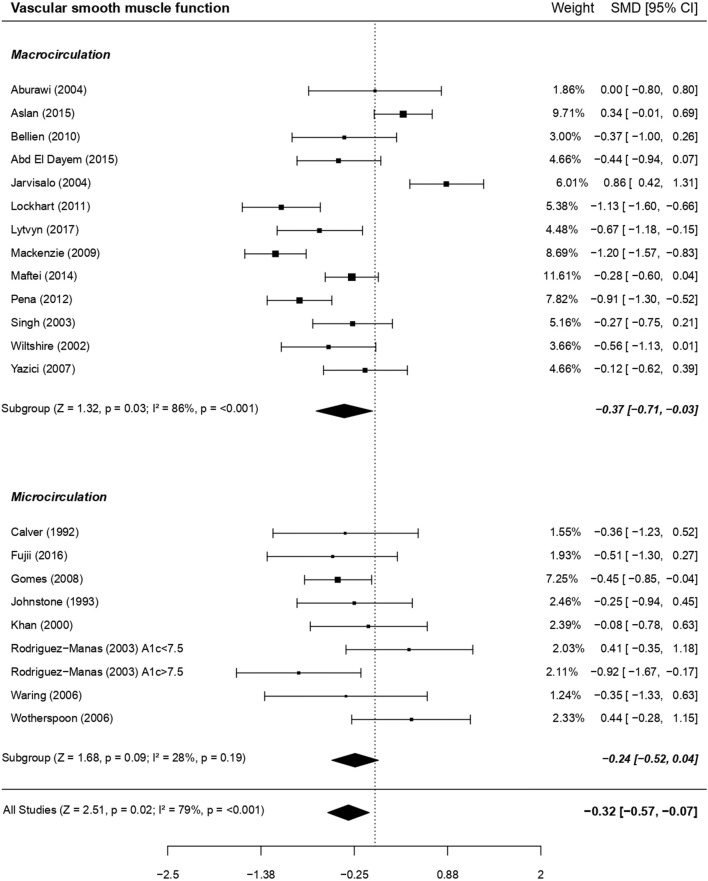
Background: A large yet heterogeneous body of literature exists suggesting that endothelial dysfunction appears early in type 1 diabetes, due to hyperglycemia-induced oxidative stress. The latter may also affect vascular smooth muscles (VSM) function, a layer albeit less frequently considered in that pathology. This meta-analysis aims at evaluating the extent, and the contributing risk factors, of early endothelial dysfunction, and of the possible concomitant VSM dysfunction, in type 1 diabetes. Methods: PubMed, Web of Sciences, Cochrane Library databases were screened from their respective inceptions until October 2019. We included studies comparing vasodilatory capacity depending or not on endothelium (i.e., endothelial function or VSM function, respectively) in patients with uncomplicated type 1 diabetes and healthy controls. Results: Fifty-eight articles studying endothelium-dependent function, among which 21 studies also assessed VSM, were included. Global analyses revealed an impairment of standardized mean difference (SMD) (Cohen's d) of endothelial function: -0.61 (95% CI: -0.79, -0.44) but also of VSM SMD: -0.32 (95% CI: -0.57, -0.07). The type of stimuli used (i.e., exercise, occlusion-reperfusion, pharmacological substances, heat) did not influence the impairment of the vasodilatory capacity. Endothelial dysfunction appeared more pronounced within macrovascular than microvascular beds. The latter was particularly altered in cases of poor glycemic control [HbA1c > 67 mmol/mol (8.3%)]. Conclusions: This meta-analysis not only corroborates the presence of an early impairment of endothelial function, even in response to physiological stimuli like exercise, but also highlights a VSM dysfunction in children and adults with type 1 diabetes. Endothelial dysfunction seems to be more pronounced in large than small vessels, fostering the debate on their relative temporal appearance.
Keywords: endothelial function; exercise; macrocirculation; microcirculation; peripheral vascular disease; smooth muscle function; type 1 diabetes.
Copyright © 2020 Lespagnol, Dauchet, Pawlak-Chaouch, Balestra, Berthoin, Feelisch, Roustit, Boissière, Fontaine and Heyman.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous