

doi: 10.11909/j.issn.1671-5411.2020.04.006.
Percutaneous recanalization of total saphenous vein graft occlusion with excimer laser treatment
Affiliations
- PMID: 32362924
- PMCID: PMC7189262
- DOI: 10.11909/j.issn.1671-5411.2020.04.006
Item in Clipboard
Percutaneous recanalization of total saphenous vein graft occlusion with excimer laser treatment
J Geriatr Cardiol.
2020 Apr.
No abstract available
Keywords: Excimer laser; Percutaneous coronary intervention; Saphenous vein graft.
Figures
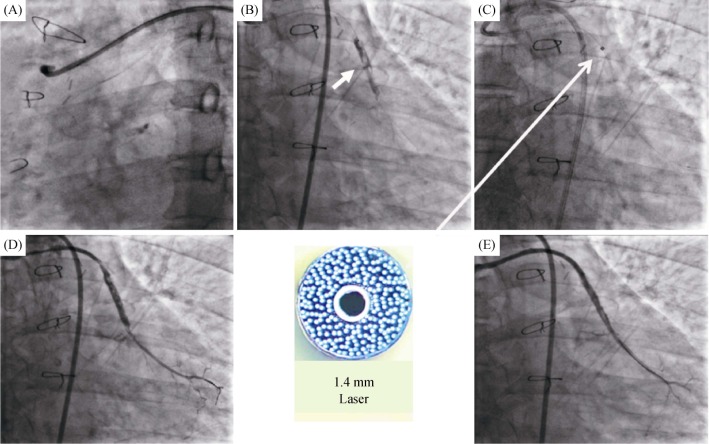
(A): Coronary angiogram showing the total occlusion of the SVG to the OM branch; (B): dye injection revealed a heavy thrombus burden (arrow); (C): the 1.4 mm laser catheter was inserted and the laser ablation was performed (arrow); and (D & E): the final angiogram. OM: obtuse marginal; SVG: saphenous vein graft.
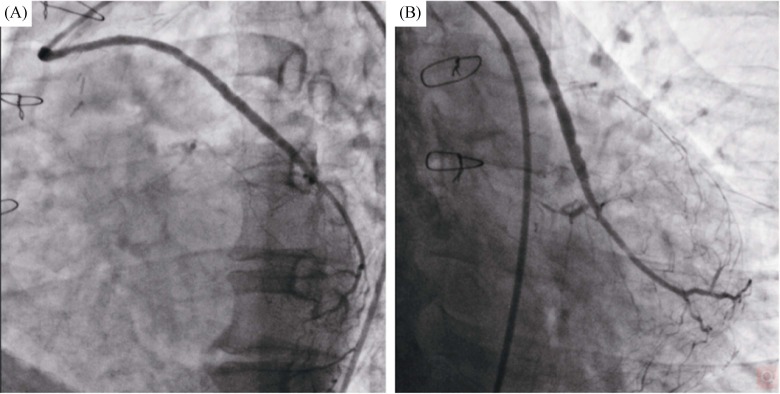
(A): The left anterior oblique 45° view of the SVG to the OM branch angiogram; and (B): the caudal view of the SVG to the OM branch angiogram. OM: obtuse marginal; SVG: saphenous vein graft.
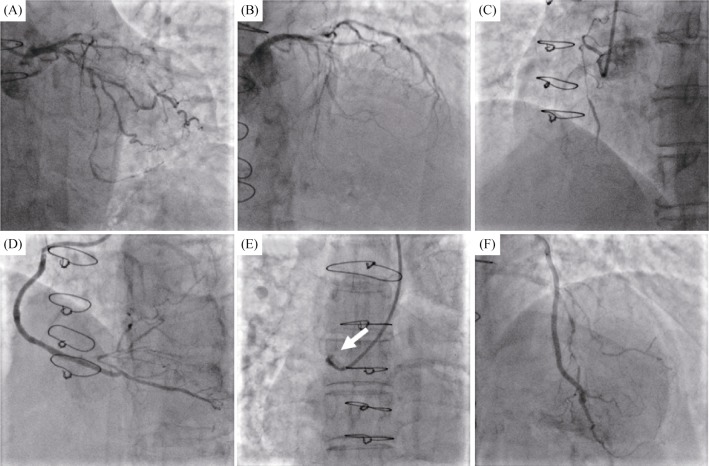
(A): The 90% stenosis with calcification in the proximal segment of the left circumflex artery; (B): the proximal segment of the LAD was total occlusion; (C): the ostial RCA were completely occluded; (D): the SVG to RCA was unobstructed; (E): the SVG to the OM branch was totally occluded (arrow); and (F): the left internal mammary artery to LAD was unobstructed. LAD: left anterior descending; OM: obtuse marginal; RCA: right coronary artery; SVG: saphenous vein graft.
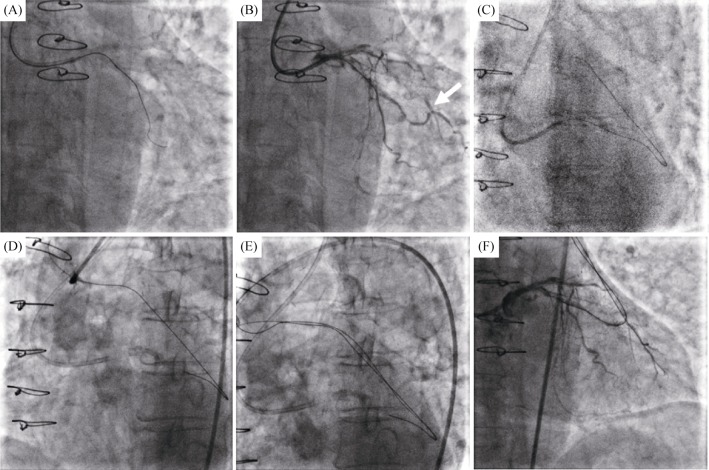
(A): Microcatheter and small balloons failed to cross the left circumflex artery lesion; (B): competitive retrograde blood flow seemed to have developed from the OM branch to the graft anastomosis (arrow); (C & D): the retrograde guidewire passed through the occlusion segment and entered into the ascending aorta; (E): the antegrade guidewire crossed the lesions to the distal OM branch under the direction of the retrograde wire; and (F): angiogram positioned the antegrade guidewire in the true lumen. OM: obtuse marginal; SVG: saphenous vein graft.
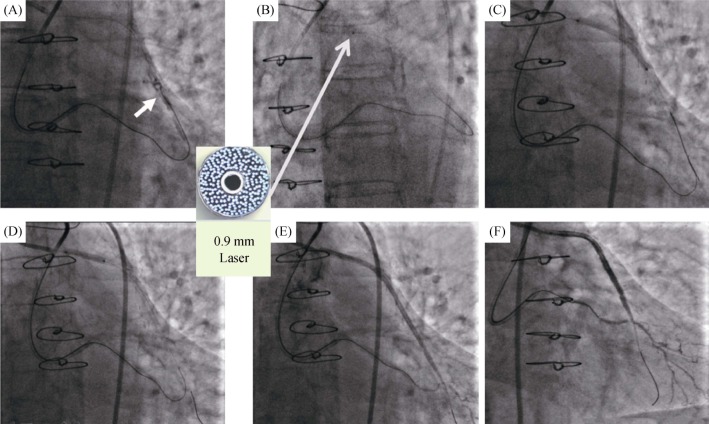
(A): Tip injection showed a large amount of thrombus in the middle of SVG (arrow); (B): ablation from the proximal to the distal SVG was performed with the 0.9 mm laser catheter (arrow); (C): two drug-eluting stents (2.75 mm × 36 mm & 3.0 mm × 33 mm) were implanted from the distal to the ostial degenerated SVG; (D): post dilation with the 3.0 mm × 12 mm noncompliant balloon; and (E & F): the final angiogram result after laser facilitated percutaneous coronary intervention. OM: obtuse marginal; SVG: saphenous vein graft.
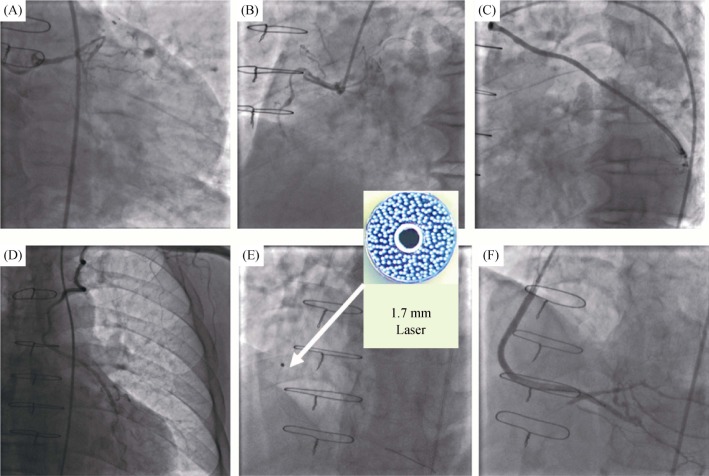
(A–D): The coronary angiogram demonstrate the LIMA to LAD and the SVG to the OM branch were unobstructed, and the SVG to the PDA was occluded; (E): the 1.7 mm laser catheter through the SVG lesions and ablation (arrow); and (F): the good angiographic results after two stents were deployed. LAD: left anterior descending; LIMA: left internal mammary artery; OM: obtuse marginal; PDA: posterior descending artery; SVG: saphenous vein graft.
References
-
- Niccoli G, Belloni F, Cosentino N, et al. Case-control registry of excimer laser coronary angioplasty versus distal protection devices in patients with acute coronary syndromes due to saphenous vein graft disease. Am J Cardiol. 2013;112:1586–1591. - PubMed
-
- Brilakis ES, O'Donnell CI, Penny W, et al. Percutaneous coronary intervention in native coronary arteries versus bypass grafts in patients with prior coronary artery bypass graft surgery: insights from the Veterans Affairs Clinical Assessment, Reporting, and Tracking program. JACC Cardiovasc Interv. 2016;9:884–893. - PubMed
-
- Brennan JM, Al-Hejily W, Dai D, et al. Three-year outcomes associated with embolic protection in saphenous vein graft intervention: results in 49325 senior patients in the Medicare-linked National Cardiovascular Data Registry Cath PCI Registry. Circ Cardiovasc Interv. 2015;8:e001403. - PubMed
-
- Fracassi F, Roberto M, Niccoli G. Current interventional coronary applications of excimer laser. Expert Rev Med Devices. 2013;10:541–549. - PubMed
-
- Ebersole D, Dahm JB, Das T, et al. Excimer laser revascularization of saphenous vein grafts in acute myocardial infarction. J Invasive Cardiol. 2004;16:177–180. - PubMed
LinkOut - more resources
Full Text Sources