

Investigational Biomarkers for Checkpoint Inhibitor Immune-Related Adverse Event Prediction and Diagnosis
- PMID: 32363387
- PMCID: PMC7259479
- DOI: 10.1093/clinchem/hvaa081
Investigational Biomarkers for Checkpoint Inhibitor Immune-Related Adverse Event Prediction and Diagnosis
Abstract
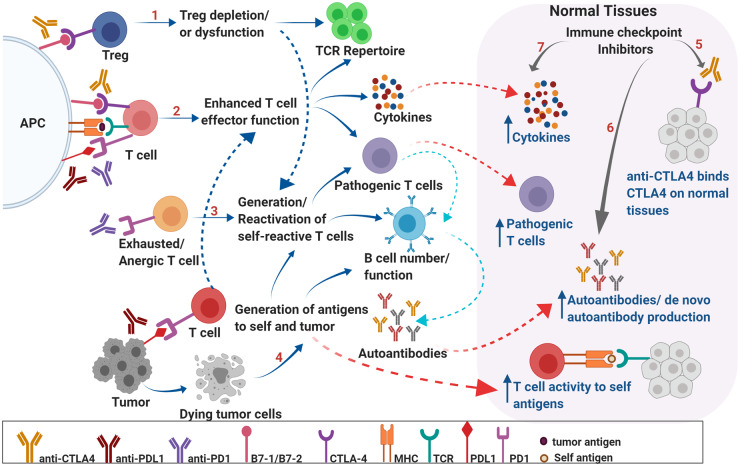
Background: Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of multiple cancers. However, these promising therapies may also cause immune-related adverse events (irAEs) in a substantial proportion of patients. These autoimmune phenomena may affect almost any organ system and may occur at almost any point in therapy. In some instances, these toxicities are life-threatening and potentially permanent. Diverse clinical presentation and unpredictable timing further complicate their anticipation and diagnosis.
Content: To improve patient safety and selection for ICI use, biomarkers for irAE diagnosis and prediction are under development. Clinicians may use traditional laboratory markers such as routine chemistries, creatinine clearance, thyroid function tests, and serum cortisol/adrenocorticotrophic hormone to monitor for specific irAEs, but noted aberrations may not necessarily represent an immune-mediated etiology. Novel biomarkers have the potential to be more specific to assist in the diagnosis of irAEs. The prediction of irAEs is more challenging. Apart from a history of autoimmune disease, no other clinical parameters are routinely used to project risk. Biomarker candidates under investigation for irAE diagnosis and prediction include blood cell analysis, chemokines/cytokines, autoantibodies, and genetic predisposition, such as human leukocyte antigen haplotype. Among other emerging candidates are immune-cell subsets, T-cell repertoire, fecal microbiome, tumor genomics, and radiomic characterization.
Summary: Several conventional laboratory indexes of end-organ dysfunction are currently in routine clinical use for irAE monitoring and diagnosis. Novel biomarkers for the prediction and diagnosis of these irAEs, which primarily characterize patient immune function, represent an area of active investigation.
© American Association for Clinical Chemistry 2020. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- US Food and Drug Administration. Drugs@FDA: FDA-approved drug products. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm (Accessed March 2020).
-
- Brahmer JR, Lacchetti C, Schneider BJ, Atkins MB, Brassil KJ, Caterino JM, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline. J Clinc Oncol 2018;36:1714–68. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
