

A Systematic Review of Methodological Variation in Healthcare Provider Perspective Tuberculosis Costing Papers Conducted in Low- and Middle-Income Settings, Using An Intervention-Standardised Unit Cost Typology
- PMID: 32363543
- PMCID: PMC7437656
- DOI: 10.1007/s40273-020-00910-w
A Systematic Review of Methodological Variation in Healthcare Provider Perspective Tuberculosis Costing Papers Conducted in Low- and Middle-Income Settings, Using An Intervention-Standardised Unit Cost Typology
Erratum in
-
Correction to: A Systematic Review of Methodological Variation in Healthcare Provider Perspective Tuberculosis Costing Papers Conducted in Low- and Middle-Income Settings, Using An Intervention-Standardised Unit Cost Typology.Pharmacoeconomics. 2020 Aug;38(8):899-900. doi: 10.1007/s40273-020-00928-0. Pharmacoeconomics. 2020. PMID: 32462638 Free PMC article.
Abstract
Background: There is a need for easily accessible tuberculosis unit cost data, as well as an understanding of the variability of methods used and reporting standards of that data.
Objective: The aim of this systematic review was to descriptively review papers reporting tuberculosis unit costs from a healthcare provider perspective looking at methodological variation; to assess quality using a study quality rating system and machine learning to investigate the indicators of reporting quality; and to identify the data gaps to inform standardised tuberculosis unit cost collection and consistent principles for reporting going forward.
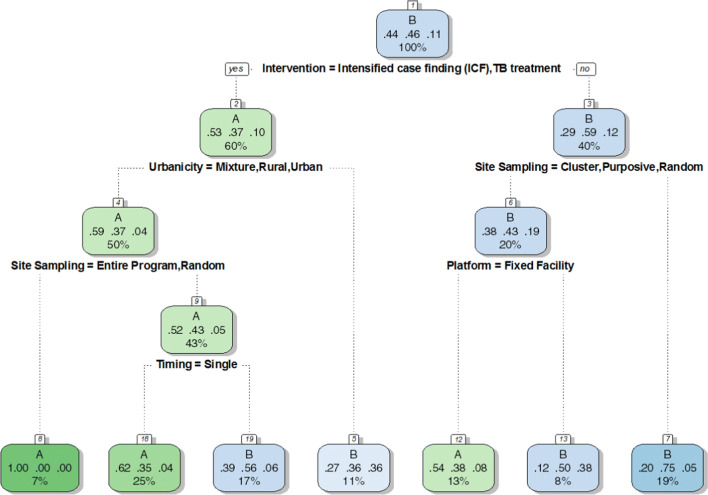
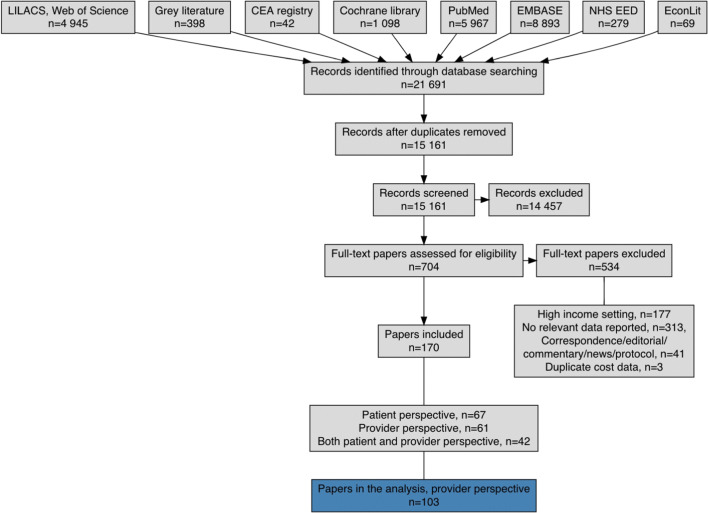
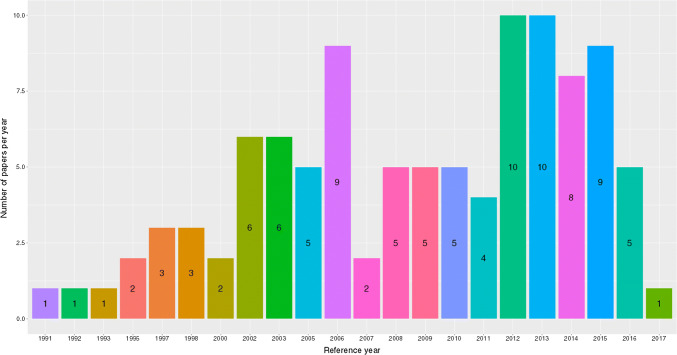
Methods: We searched grey and published literature in five sources and eight databases, respectively, using search terms linked to cost, tuberculosis and tuberculosis health services including tuberculosis treatment and prevention. For inclusion, the papers needed to contain empirical unit cost estimates for tuberculosis interventions from low- and middle-income countries, with reference years between 1990 and 2018. A total of 21,691 papers were found and screened in a phased manner. Data were extracted from the eligible papers into a detailed Microsoft Excel tool, extensively cleaned and analysed with R software (R Project, Vienna, Austria) using the user interface of RStudio. A study quality rating was applied to the reviewed papers based on the inclusion or omission of a selection of variables and their relative importance. Following this, machine learning using a recursive partitioning method was utilised to construct a classification tree to assess the reporting quality.
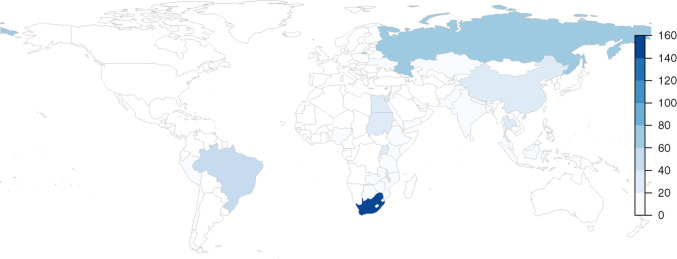
Results: This systematic review included 103 provider perspective papers with 627 unit costs (costs not presented here) for tuberculosis interventions among a total of 140 variables. The interventions covered were active, passive and intensified case finding; tuberculosis treatment; above-service costs; and tuberculosis prevention. Passive case finding is the detection of tuberculosis cases where individuals self-identify at health facilities; active case finding is detection of cases of those not in health facilities, such as through outreach; and intensified case finding is detection of cases in high-risk populations. There was heterogeneity in some of the reported methods used such cost allocation, amortisation and the use of top-down, bottom-up or mixed approaches to the costing. Uncertainty checking through sensitivity analysis was only reported on by half of the papers (54%), while purposive and convenience sampling was reported by 72% of papers. Machine learning indicated that reporting on 'Intervention' (in particular), 'Urbanicity' and 'Site Sampling', were the most likely indicators of quality of reporting. The largest data gap identified was for tuberculosis vaccination cost data, the Bacillus Calmette-Guérin (BCG) vaccine in particular. There is a gap in available unit costs for 12 of 30 high tuberculosis burden countries, as well as for the interventions of above-service costs, tuberculosis prevention, and active and intensified case finding.
Conclusion: Variability in the methods and reporting used makes comparison difficult and makes it hard for decision makers to know which unit costs they can trust. The study quality rating system used in this review as well as the classification tree enable focus on specific reporting aspects that should improve variability and increase confidence in unit costs. Researchers should endeavour to be explicit and transparent in how they cost interventions following the principles as laid out in the Global Health Cost Consortium's Reference Case for Estimating the Costs of Global Health Services and Interventions, which in turn will lead to repeatability, comparability and enhanced learning from others.
Conflict of interest statement
The authors declare no conflicts, financial or otherwise.
Figures
References
-
- Global tuberculosis report 2018. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
-
- Vassall A, Sweeney S, Kahn JG, Gomez G, Bollinger L, Marseille E, et al. Reference Case for Estimating the Costs of Global Health Services and Interventions. Global Health Cost Consortium; 2017.
-
- Cunnama L, Garcia Baena I, Gomez G, Laurence Y, Levin C, Siapka M, et al. Costing guidelines for tuberculosis interventions. 2019. Licence: CC BY-NC-SA 3.0 IGO.
-
- DeCormier Plosky W, Bollinger L, Alexander L, Cameron D, Carroll LN, Gomez GB, et al. Developing the Global Health Cost Consortium Unit Cost Study Repository for HIV and TB: methodology and lessons learned. Afr J AIDS Res. 2019;18(4):263–276. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
