Comparison Between Rituximab Treatment for New-Onset Generalized Myasthenia Gravis and Refractory Generalized Myasthenia Gravis
- PMID: 32364568
- PMCID: PMC7199182
- DOI: 10.1001/jamaneurol.2020.0851
Comparison Between Rituximab Treatment for New-Onset Generalized Myasthenia Gravis and Refractory Generalized Myasthenia Gravis
Abstract
Importance: Use of biologic agents in generalized myasthenia gravis is generally limited to therapy-refractory cases; benefit in new-onset disease is unknown.
Objective: To assess rituximab in refractory and new-onset generalized myasthenia gravis and rituximab vs conventional immunotherapy in new-onset disease.
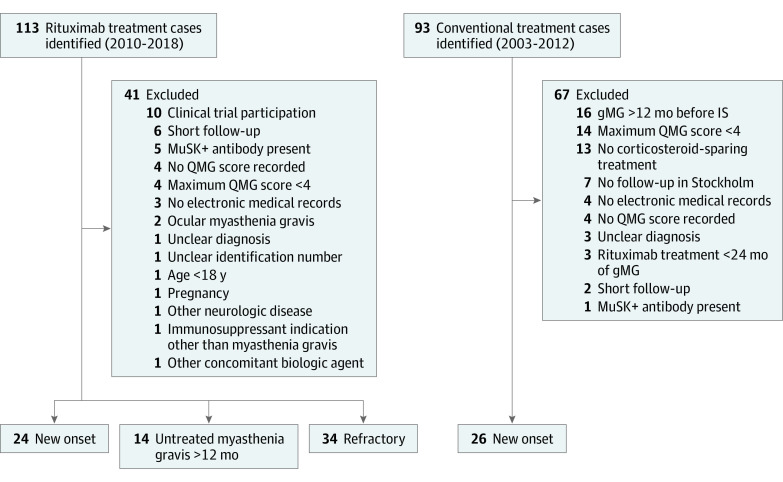
Design, setting, and participants: A retrospective cohort study with prospectively collected data was conducted on a county-based community sample at Karolinska University Hospital, Stockholm, Sweden. Participants included 72 patients with myasthenia gravis, excluding those displaying muscle-specific tyrosine kinase antibodies, initiating rituximab treatment from January 1, 2010, to December 31, 2018, and patients with new-onset disease initiating conventional immunotherapy from January 1, 2003, to December 31, 2012, with 12 months or more of observation time. The present study was conducted from March 1, 2019, to January 31, 2020.
Exposures: Treatment with low-dose rituximab (most often 500 mg every 6 months) or conventional immunosuppressants.
Main outcomes and measures: Time to remission (main outcome) as well as use of rescue therapies or additional immunotherapies and time in remission (secondary outcomes).
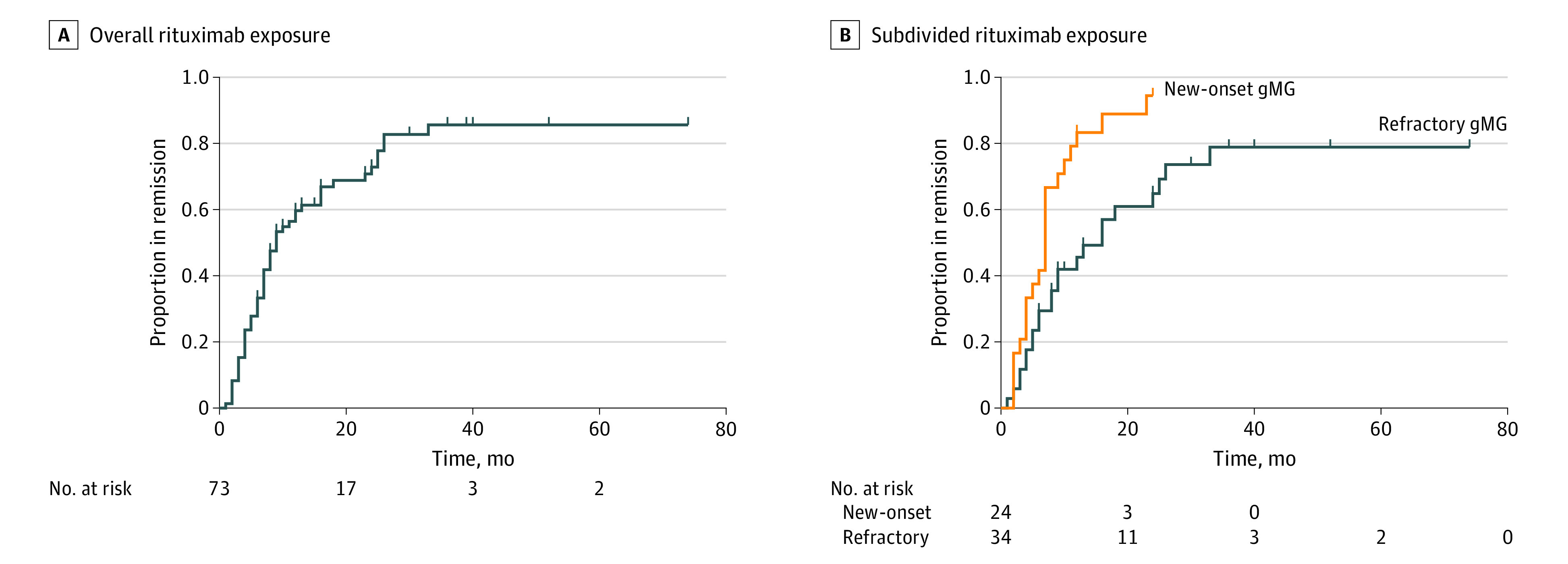
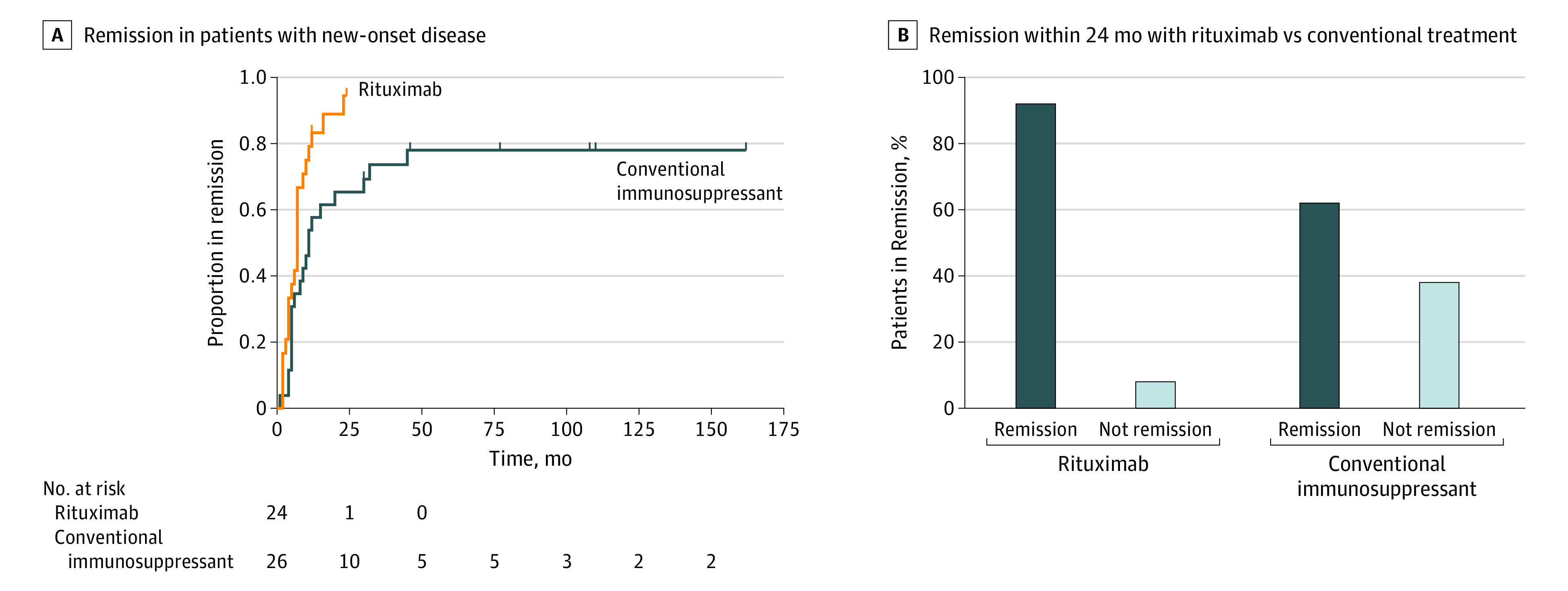
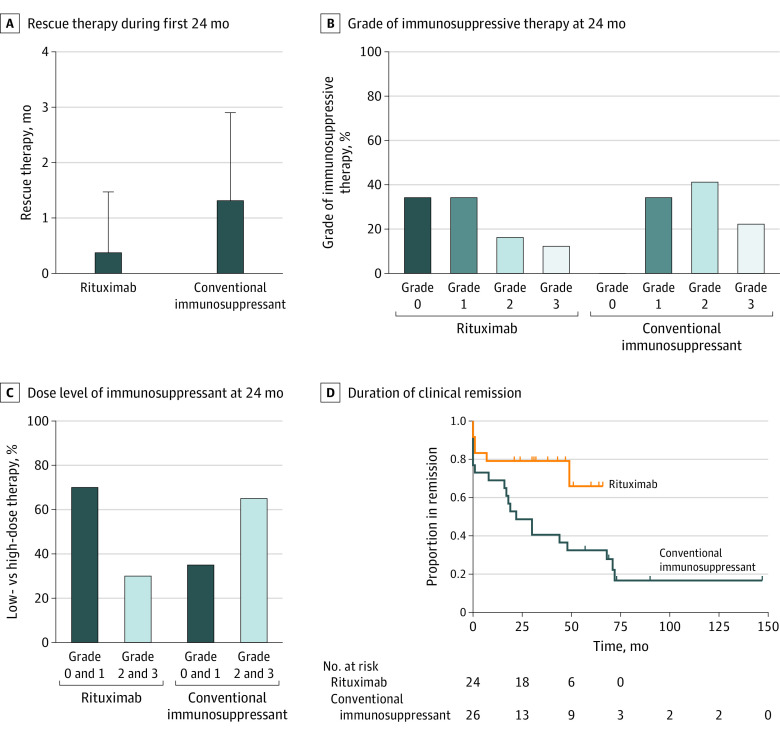
Results: Of the 72 patients included, 31 patients (43%) were women; mean (SD) age at treatment start was 60 (18) years. Twenty-four patients had received rituximab within 12 months of disease onset and 48 received rituximab at a later time, 34 of whom had therapy-refractory disease. A total of 26 patients (3 [12%] women; mean [SD] age, 68 [11] years at treatment start) received conventional immunosuppressant therapy. Median time to remission was shorter for new-onset vs refractory disease (7 vs 16 months: hazard ratio [HR], 2.53; 95% CI, 1.26-5.07; P = .009 after adjustment for age, sex, and disease severity) and for rituximab vs conventional immunosuppressant therapies (7 vs 11 months: HR, 2.97; 95% CI, 1.43-6.18; P = .004 after adjustment). In addition, fewer rescue therapy episodes during the first 24 months were required (mean [SD], 0.38 [1.10] vs 1.31 [1.59] times; mean difference, -1.26; 95% CI, -1.97 to -0.56; P < .001 after adjustment), and a larger proportion of patients had minimal or no need of additional immunotherapies (70% vs 35%; OR, 5.47; 95% CI, 1.40-21.43; P = .02 after adjustment). Rates of treatment discontinuation due to adverse events were lower with rituximab compared with conventional therapies (3% vs 46%; P < .001 after adjustment).
Conclusions and relevance: Clinical outcomes with rituximab appeared to be more favorable in new-onset generalized myasthenia gravis, and rituximab also appeared to perform better than conventional immunosuppressant therapy. These findings suggest a relatively greater benefit of rituximab earlier in the disease course. A placebo-controlled randomized trial to corroborate these findings is warranted.
Conflict of interest statement
Figures