

Evaluating the Risk of Macrovascular Events and Mortality Among People With Multiple Sclerosis in England
- PMID: 32364569
- PMCID: PMC7199174
- DOI: 10.1001/jamaneurol.2020.0664
Evaluating the Risk of Macrovascular Events and Mortality Among People With Multiple Sclerosis in England
Abstract
Importance: People with multiple sclerosis (MS) are associated with an increased risk of cardiovascular disease and mortality; however, evidence from population-based studies is sparse.
Objective: To assess whether the risk of macrovascular events and mortality differs among people with MS compared with a matched population without MS in England.
Design, setting, and participants: A population-based retrospective matched cohort study was conducted in general practices registered with the Clinical Practice Research Datalink in England between January 1, 1987, and September 30, 2018, with a mean (SD) follow-up of 11.3 (6.5) years. A total of 12 251 patients with MS were matched with up to 6 people without MS (n = 72 572) by age, sex, and general practice. People with 3 or more diagnoses of MS recorded during the study period were included. The first MS diagnosis was considered as index date.
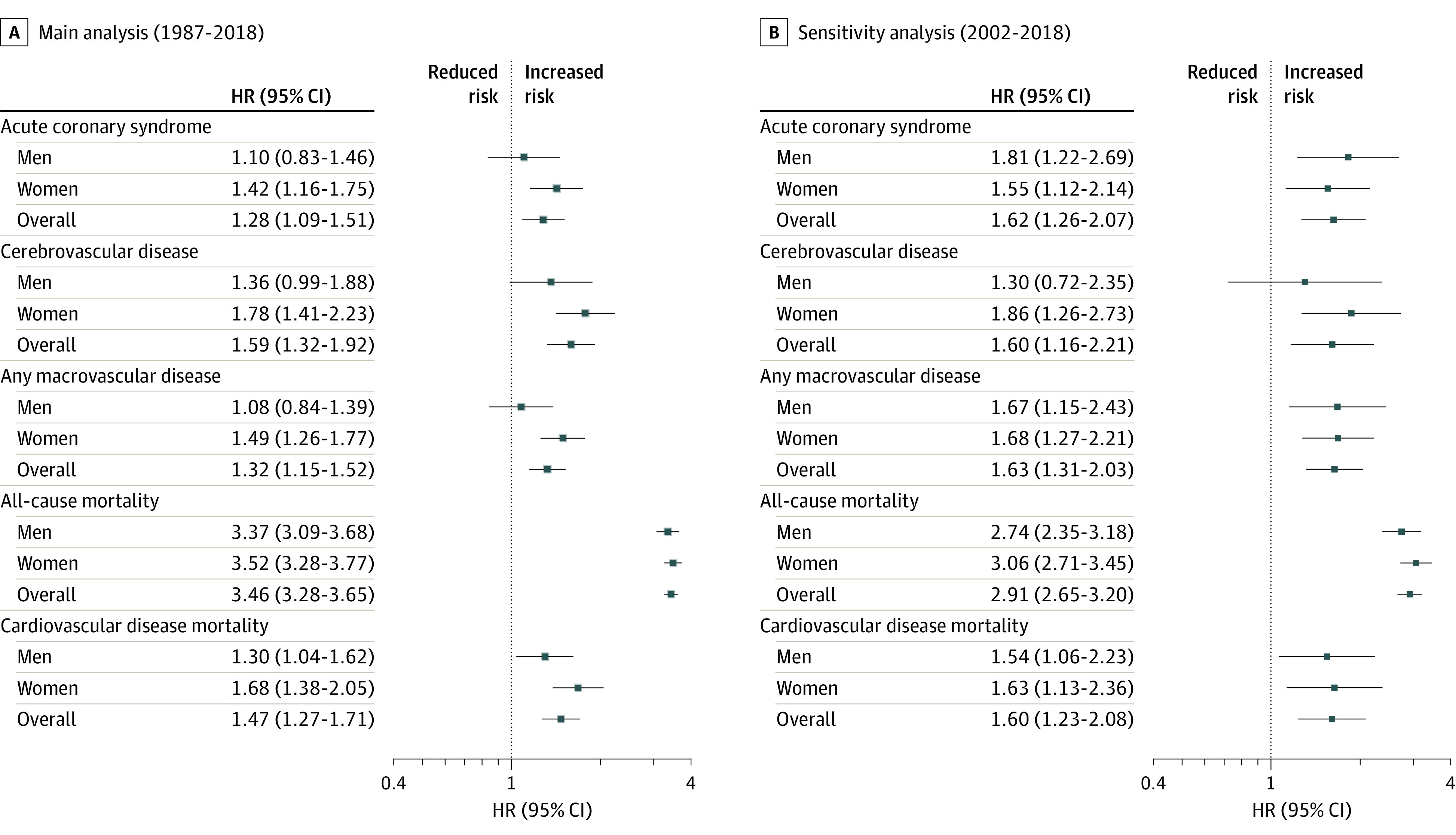
Exposures: Multiple sclerosis status. Analyses were also stratified by sex.
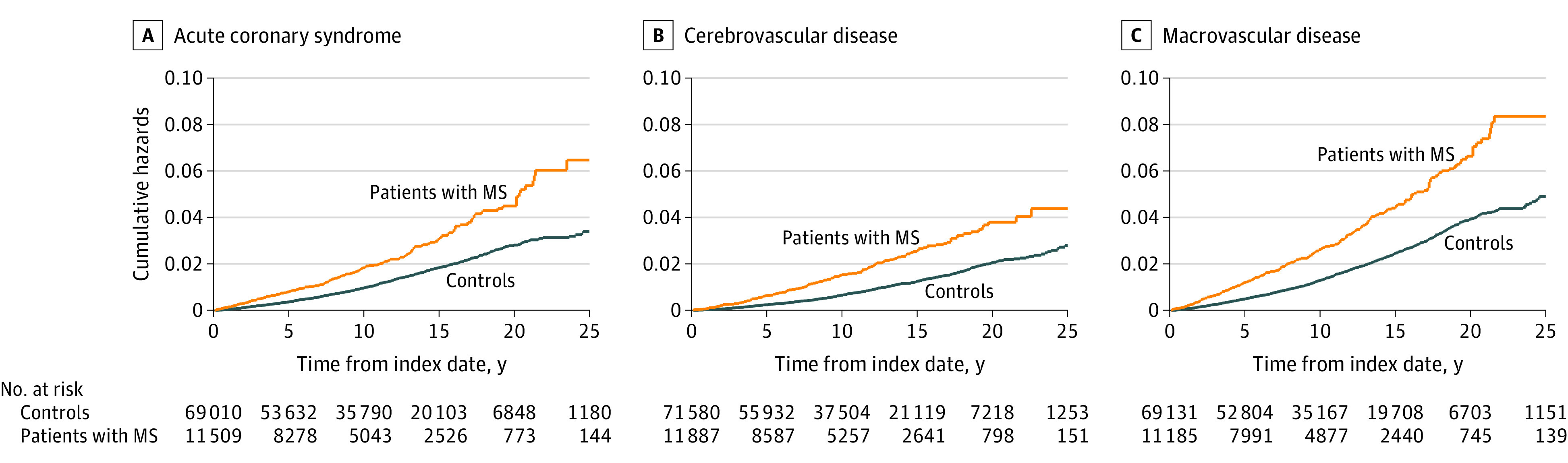
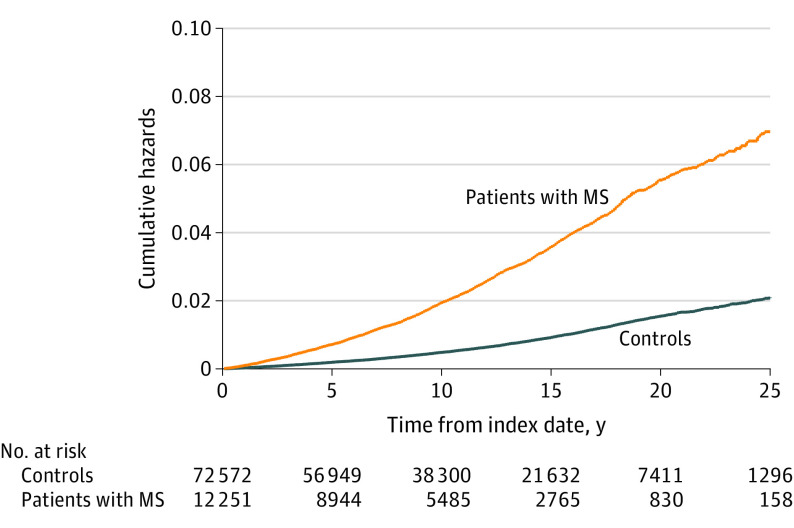
Main outcomes and measures: Main outcomes were acute coronary syndrome, cerebrovascular disease, any macrovascular disease (including peripheral arterial disease), and mortality (all-cause mortality and cardiovascular disease-specific mortality). Cox proportional hazards regression and Fine and Gray proportional subhazard regression models were used to assess differences in rates.
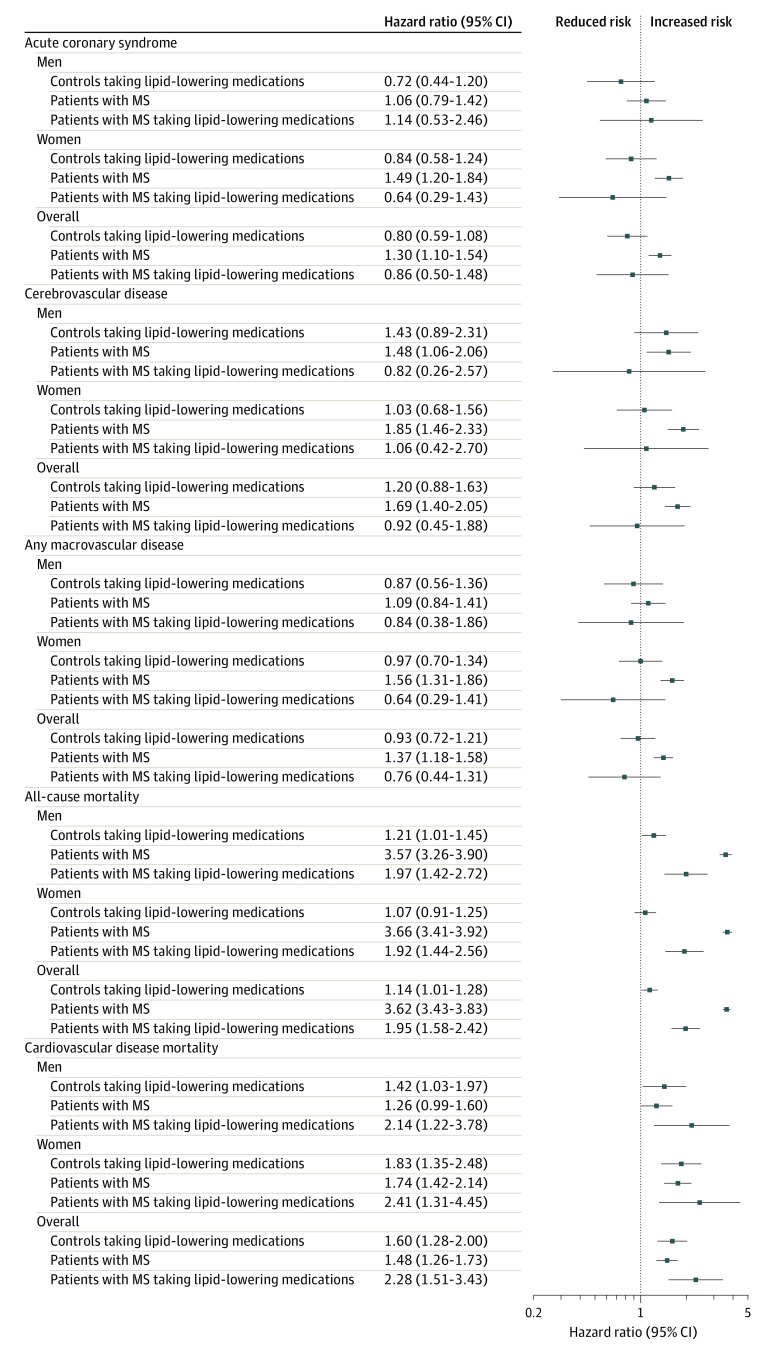
Results: A total of 12 251 people with MS (66.9% women; mean [SD] age, 44.9 [13.3] years) were matched with 72 572 people without MS (69.8% women; mean [SD] age, 44.9 [13.3] years). As compared with people without MS, people with MS were associated with a 28% increased hazard of acute coronary syndrome (hazard ratio [HR], 1.28; 95% CI, 1.09-1.51), 59% increased hazard of cerebrovascular disease (HR, 1.59; 95% CI, 1.32-1.92), 32% increased hazard of any macrovascular disease (HR, 1.32; 95% CI, 1.15-1.52), 3.5-fold increased hazard of all-cause mortality (HR, 3.46; 95% CI, 3.28-3.65), and 1.5-fold increased hazard in cardiovascular disease mortality (HR, 1.47; 95% CI, 1.27-1.71). Differences in macrovascular events were more pronounced among women than men. Mortality risk was also higher for women than men. Treatment with lipid-lowering medications (mainly statins) was associated with lower mortality rates among people with MS.
Conclusions and relevance: This study suggests that MS is associated with an increased risk of cardiovascular and cerebrovascular disease that is not completely accounted for by traditional vascular risk factors. Given the adverse effects of these comorbidities on outcomes in patients with MS, further investigation is needed.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
