

Trends Among Rural and Urban Medicare Beneficiaries in Care Delivery and Outcomes for Acute Stroke and Transient Ischemic Attacks, 2008-2017
- PMID: 32364573
- PMCID: PMC7358912
- DOI: 10.1001/jamaneurol.2020.0770
Trends Among Rural and Urban Medicare Beneficiaries in Care Delivery and Outcomes for Acute Stroke and Transient Ischemic Attacks, 2008-2017
Abstract
Importance: Over the last decade or so, there have been substantial investments in the development of stroke systems of care to improve access and quality of care in rural communities. Whether these have narrowed rural-urban disparities in care is unclear.
Objective: To describe trends among rural and urban patients with acute ischemic stroke or transient ischemic attack in the type of health care centers to which patients were admitted, what care was provided, and the outcomes patients experienced.
Design, setting, and participants: This descriptive observational study included 100% claims for beneficiaries of traditional fee-for-service Medicare from 2008 through 2017. All rural and urban areas in the US were included, defined by whether a beneficiary's residential zip code was in a metropolitan or nonmetropolitan area. All admissions in the US among patients with traditional Medicare who had a transient ischemic attack or acute stroke (N = 4.01 million) were eligible to be included in this study. Admissions for beneficiaries with end-stage kidney disease (n = 85 927 [2.14%]), beneficiaries with unidentified Rural-Urban Commuting Area codes (n = 12 797 [0.32%]), and beneficiaries not continuously enrolled in traditional Medicare in the 12 months before and 3 months after their admission (n = 442 963 [11.0%]) were excluded.
Exposures: Residence in an urban or rural area; admission to a hospital with a transient ischemic attack or acute stroke.
Main outcomes and measures: Discharge from a certified stroke center, receiving a neurology consultation during admission, treatment with alteplase, days institutionalized, and 90-day mortality.
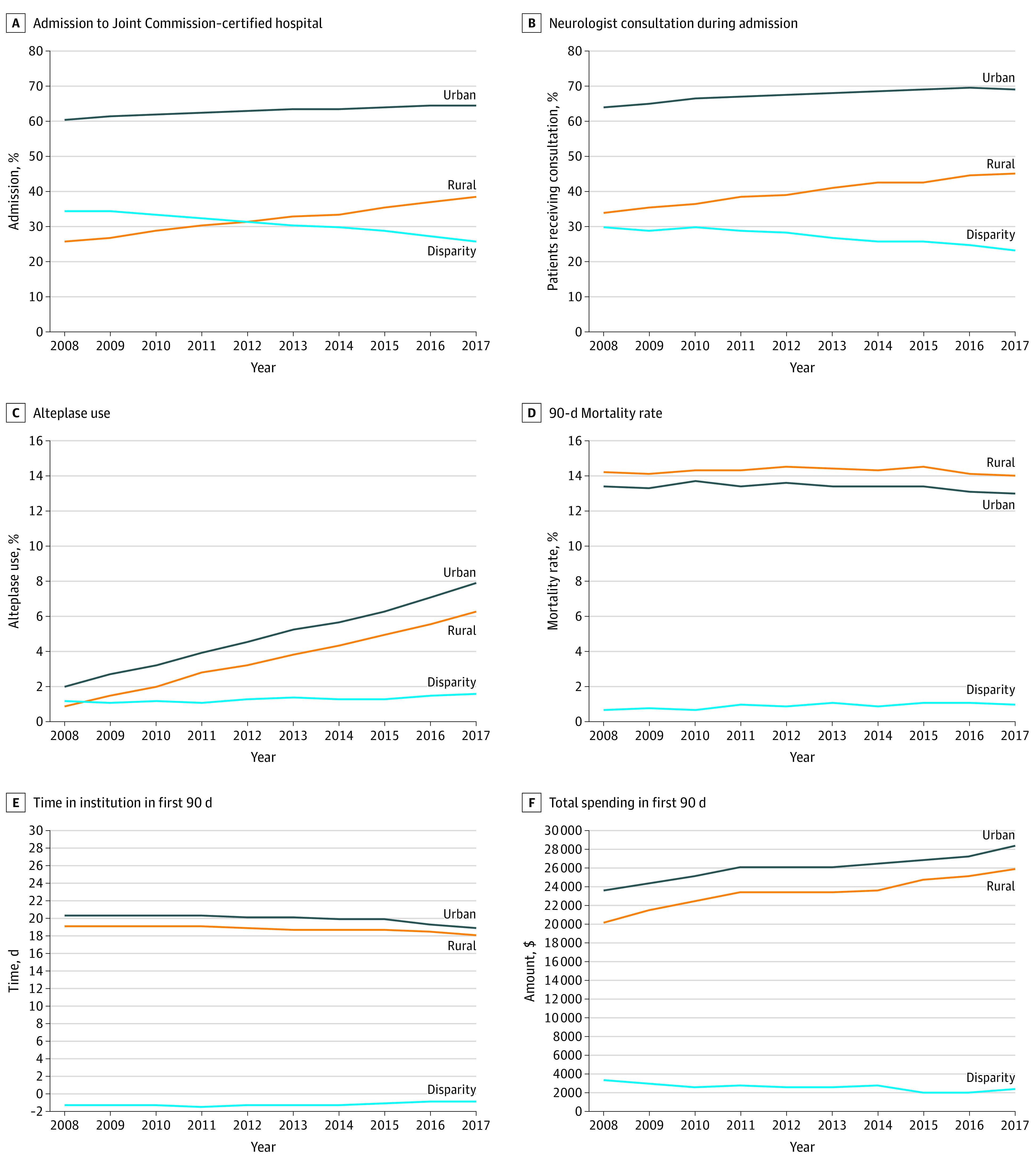
Results: The final sample included 3.47 million admissions from 2008 through 2017. In this sample, 2.01 million patients (58.0%) were female, and the mean (SD) age was 78.6 (10.5) years. In 2008, 24 681 patients (25.2%) and 161 217 patients (60.6%) in rural and urban areas, respectively, were cared for at a certified stroke center (disparity, -35.4%). By 2017, this disparity was -26.6%, having narrowed by 8.7 percentage points (95% CI, 6.6-10.8 percentage points). There was also narrowing in the rural-urban disparity in neurologist evaluation during admission (6.3% [95% CI, 4.2%-8.4%]). However, the rural-urban disparity widened or was similar with regard to receiving alteplase (0.5% [95% CI, 0.1%-0.8%]), mean days in an institution from admission (0.5 [95% CI, 0.2-0.8] days), and mortality at 90 days (0.3% [95% CI, -0.02% to 0.6%]), respectively.
Conclusions and relevance: In the last decade, care for rural residents with acute ischemic stroke and transient ischemic attack has shifted to certified stroke centers and now more likely includes neurologist input. However, disparities in access to treatments, such as alteplase, and outcomes persist, highlighting that work still is needed to extend improvements in stroke care to all US residents.
Conflict of interest statement
Figures
References
-
- Sergeev AV. Racial and rural-urban disparities in stroke mortality outside the Stroke Belt. Ethn Dis. 2011;21(3):307-313. - PubMed
-
- Ingram DD, Montresor-Lopez JA Differences in stroke mortality among adults aged 45 and over: United States, 2010–2013; NCHS data brief, no 207, July 2015. Published July 2015. Accessed March 20, 2020. https://www.cdc.gov/nchs/products/databriefs/db207.htm - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
