

Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine
- PMID: 32365488
- PMCID: PMC7290808
- DOI: 10.3390/cells9051097
Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine
Abstract
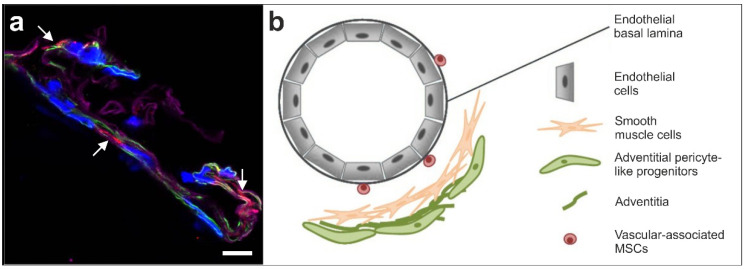
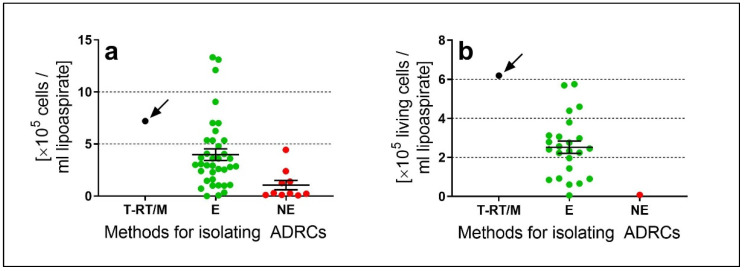
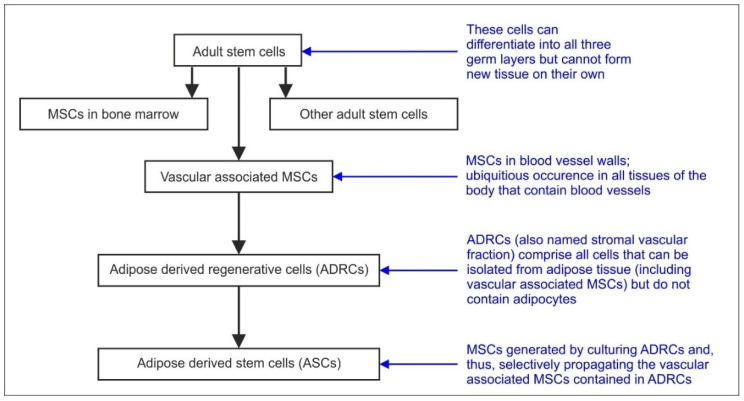
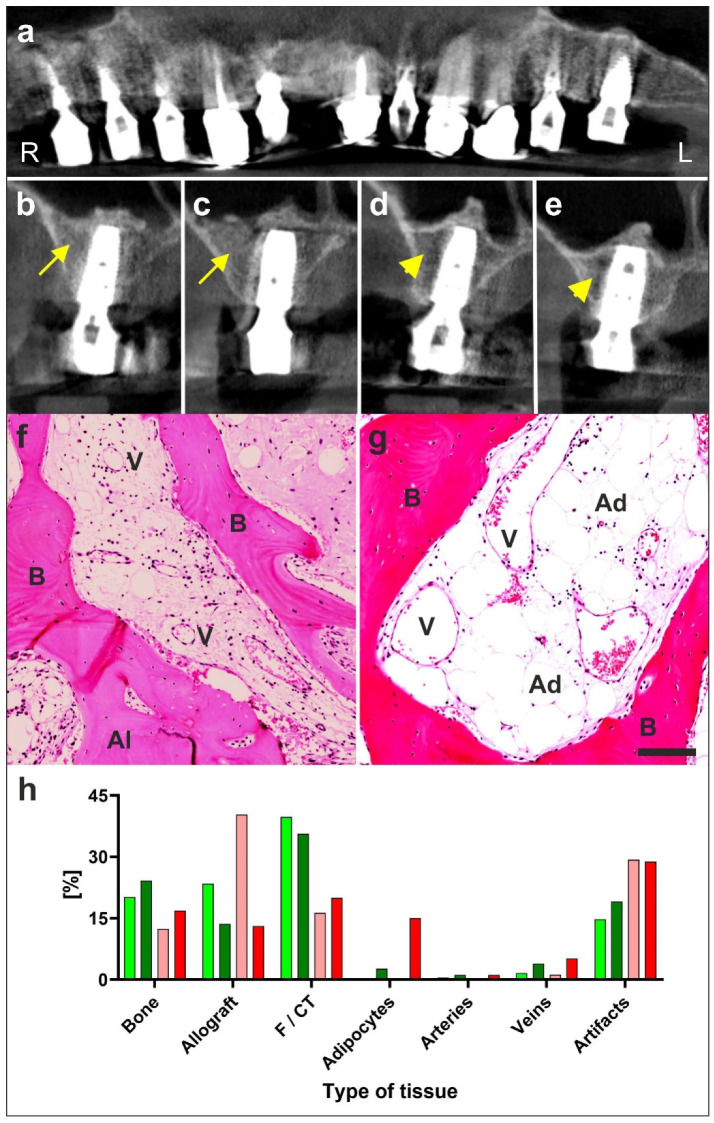
It has become practically impossible to survey the literature on cells derived from adipose tissue for regenerative medicine. The aim of this paper is to provide a comprehensive and translational understanding of the potential of UA-ADRCs (uncultured, unmodified, fresh, autologous adipose derived regenerative cells isolated at the point of care) and its application in regenerative medicine. We provide profound basic and clinical evidence demonstrating that tissue regeneration with UA-ADRCs is safe and effective. ADRCs are neither 'fat stem cells' nor could they exclusively be isolated from adipose tissue. ADRCs contain the same adult stem cells ubiquitously present in the walls of blood vessels that are able to differentiate into cells of all three germ layers. Of note, the specific isolation procedure used has a significant impact on the number and viability of cells and hence on safety and efficacy of UA-ADRCs. Furthermore, there is no need to specifically isolate and separate stem cells from the initial mixture of progenitor and stem cells found in ADRCs. Most importantly, UA-ADRCs have the physiological capacity to adequately regenerate tissue without need for more than minimally manipulating, stimulating and/or (genetically) reprogramming the cells for a broad range of clinical applications. Tissue regeneration with UA-ADRCs fulfills the criteria of homologous use as defined by the regulatory authorities.
Keywords: ADRCs; adipose tissue derived regenerative cells; efficacy; point of care treatment; randomized controlled trials; review; safety; stem cells; stromal vascular fraction.
Conflict of interest statement
E.A. is Executive Chair of InGeneron, Inc. (Houston, TX, USA). G.W. is employed as Chief Scientific Officer at InGeneron, Inc. C.A. is Director Medical and Regulatory Affairs (Munich, Germany) which is owned by InGeneron, Inc. C.S. serves as consultant to InGeneron, Inc. A.H. declares no conflict of interest. InGeneron, Inc. and InGeneron, GmbH had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Davidoff M.S. The pluripotent microvascular pericytes are the adult stem cells even in the testis. Adv. Exp. Med. Biol. 2019;1122:235–267. - PubMed
-
- Stem Cell Key Terms. [(accessed on 16 April 2020)]; Available online: https://www.cirm.ca.gov/patients/stem-cell-key-terms.
-
- Alt E.U., Schmitz C., Bai X. Fundamentals of stem cells: Why and how patients’ own adult stem cells are the next generation of medicine. In: Trafny T., Spiri S., editors. Bioethics and Research on Adult Stem Cells. IF Press Pontifical Council for Culture; Rome, Italy: 2020. in press.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
