

Beta-blocker efficacy across different cardiovascular indications: an umbrella review and meta-analytic assessment
- PMID: 32366251
- PMCID: PMC7199339
- DOI: 10.1186/s12916-020-01564-3
Beta-blocker efficacy across different cardiovascular indications: an umbrella review and meta-analytic assessment
Abstract
Background: Beta-blockers are widely used for many cardiovascular conditions; however, their efficacy in contemporary clinical practice remains uncertain.
Methods: We performed a prospectively designed, umbrella review of meta-analyses of randomised controlled trials (RCTs) investigating the evidence of beta-blockers in the contemporary management of coronary artery disease (CAD), heart failure (HF), patients undergoing surgery or hypertension (registration: PROSPERO CRD42016038375). We searched MEDLINE, EMBASE and the Cochrane Library from inception until December 2018. Outcomes were analysed as beta-blockers versus control for all-cause mortality, myocardial infarction (MI), incident HF or stroke. Two independent investigators abstracted the data, assessed the quality of the evidence and rated the certainty of evidence.
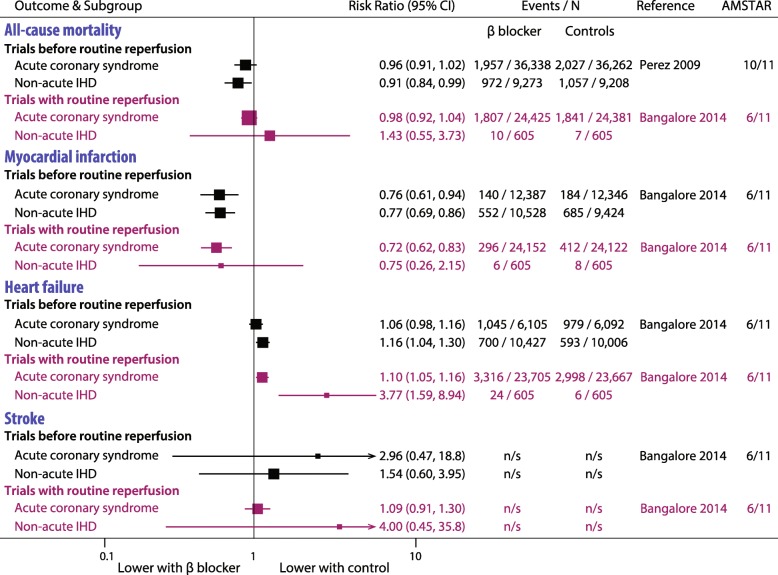
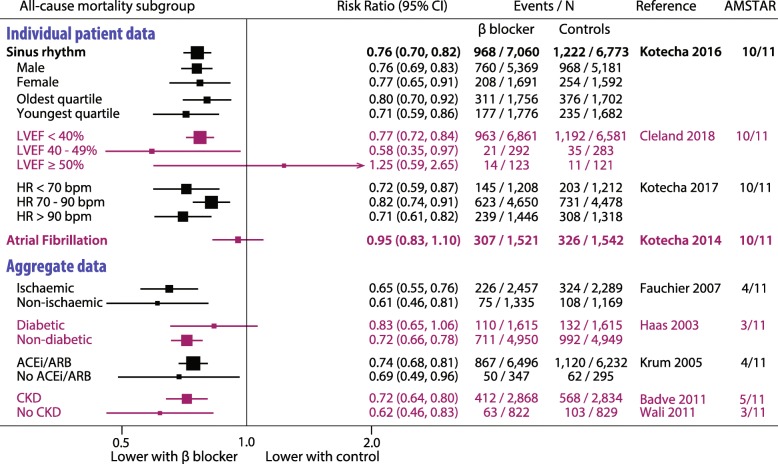
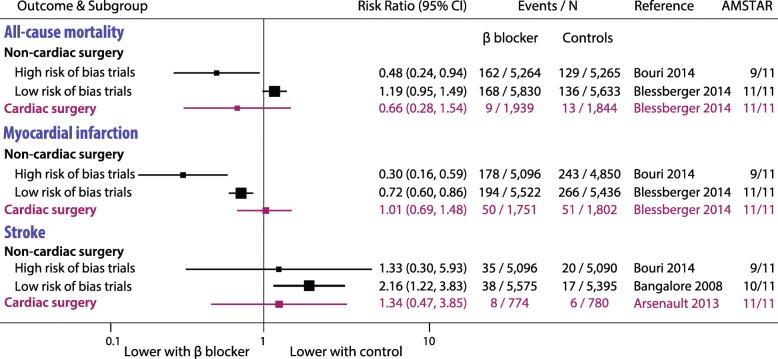
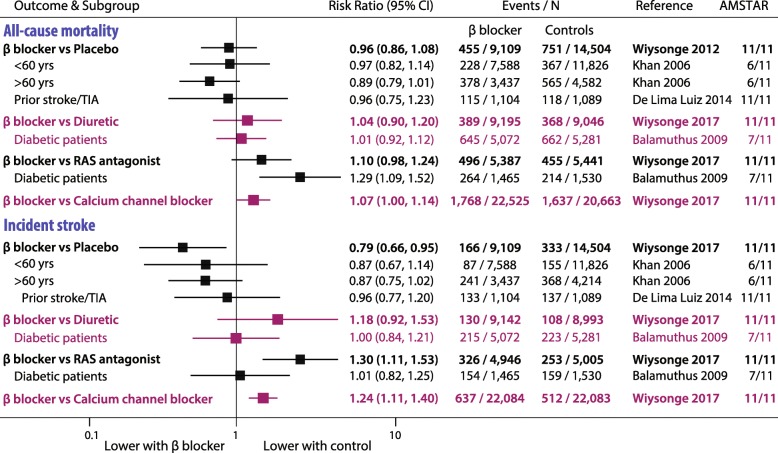
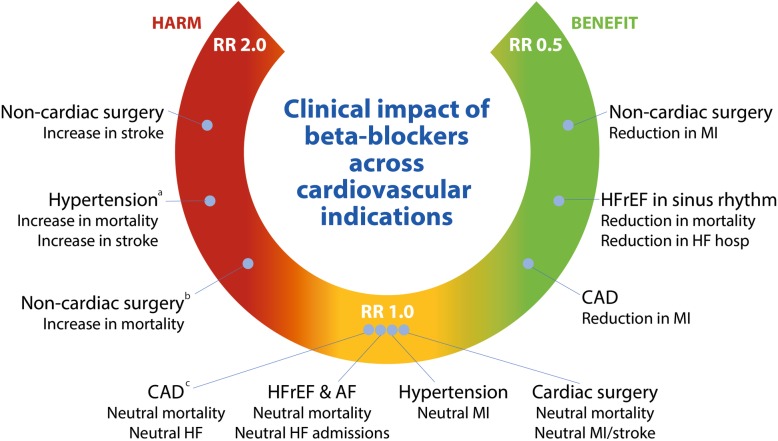
Results: We identified 98 meta-analyses, including 284 unique RCTs and 1,617,523 patient-years of follow-up. In CAD, 12 meta-analyses (93 RCTs, 103,481 patients) showed that beta-blockers reduced mortality in analyses before routine reperfusion, but there was a lack of benefit in contemporary studies where ≥ 50% of patients received thrombolytics or intervention. Beta-blockers reduced incident MI at the expense of increased HF. In HF with reduced ejection fraction, 34 meta-analyses (66 RCTs, 35,383 patients) demonstrated a reduction in mortality and HF hospitalisation with beta-blockers in sinus rhythm, but not in atrial fibrillation. In patients undergoing surgery, 23 meta-analyses (89 RCTs, 19,211 patients) showed no effect of beta-blockers on mortality for cardiac surgery, but increased mortality in non-cardiac surgery. In non-cardiac surgery, beta-blockers reduced MI after surgery but increased the risk of stroke. In hypertension, 27 meta-analyses (36 RCTs, 260,549 patients) identified no benefit versus placebo, but beta-blockers were inferior to other agents for preventing mortality and stroke.
Conclusions: Beta-blockers substantially reduce mortality in HF patients in sinus rhythm, but for other conditions, clinicians need to weigh up both benefit and potential risk.
Keywords: Coronary artery disease; Heart failure; Hypertension; Meta-analysis; Mortality; Myocardial infarction; Perioperative; Stroke; Systematic review.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form and declare the following: OJZ, MS, JPH, DIB and DPF have no relevant conflicts. FR received as direct personal payment speaker fees, honoraria, consultancy, advisory board fees, investigator, committee member from Amgen, Boehringer Ingelheim Novartis, Pfizer, BMS, Servier, Sanofi Aventis, Zoll Medical, St. Jude Medical, Fresenius Nutrition, Vifor International, Cardiorentis and Heartware and as payment to institution speaker fees, honoraria, consultancy, advisory board fees, investigator, committee member from Bayer, Novartis and St. Jude Medical. DK reports grants from Menarini and personal fees from Bayer, Atricure, Myokardia and Amomed, all outside the submitted work, and is the Chief Investigator of the RATE-AF clinical trial (NCT02391337), Steering Group Lead for the Beta-Blockers in Heart Failure Collaborative Group (BB-meta-HF; NCT NCT00832442), and a member of the consortium for an EU/EFPIA Innovative Medicines Initiative on big data for ACS/AF/HF (116074; BigData@Heart).
Figures
References
-
- Kotecha D, Manzano L, Krum H, Rosano G, Holmes J, Altman DG, Collins PD, Packer M, Wikstrand J, Coats AJ, et al. Effect of age and sex on efficacy and tolerability of beta blockers in patients with heart failure with reduced ejection fraction: individual patient data meta-analysis. BMJ. 2016;353:i1855. doi: 10.1136/bmj.i1855. - DOI - PMC - PubMed
-
- Barron AJ, Zaman N, Cole GD, Wensel R, Okonko DO, Francis DP. Systematic review of genuine versus spurious side-effects of beta-blockers in heart failure using placebo control: recommendations for patient information. Int J Cardiol. 2013;168(4):3572–3579. doi: 10.1016/j.ijcard.2013.05.068. - DOI - PMC - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):529–555. doi: 10.1161/CIR.0b013e3182742c84. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
