

The impact of sex and gender on immunotherapy outcomes
- PMID: 32366281
- PMCID: PMC7197158
- DOI: 10.1186/s13293-020-00301-y
The impact of sex and gender on immunotherapy outcomes
Abstract
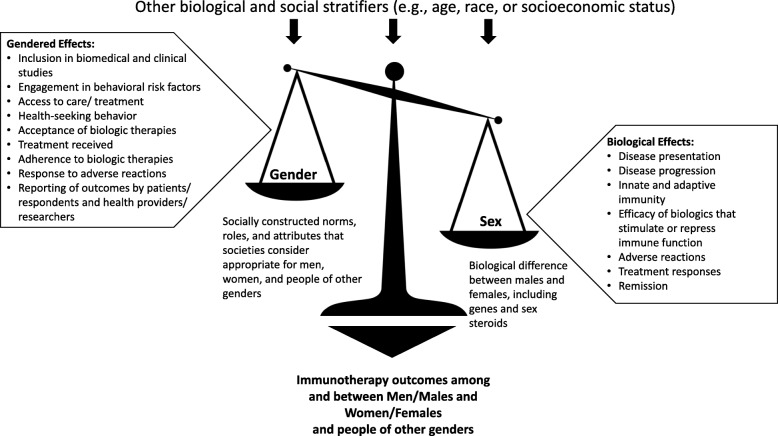
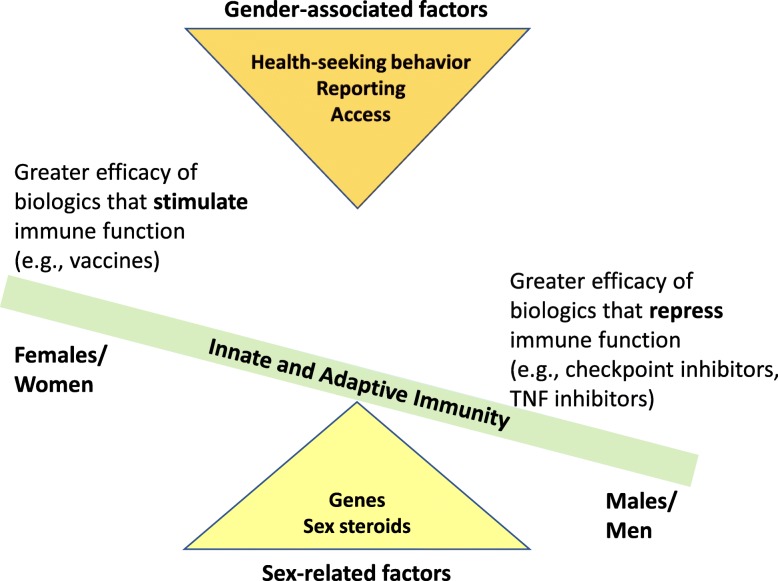
Immunotherapies are often used for the treatment, remission, and possible cure of autoimmune diseases, infectious diseases, and cancers. Empirical evidence illustrates that females and males differ in outcomes following the use of biologics for the treatment of autoimmune diseases, e.g., rheumatoid arthritis (RA), infectious diseases, e.g., influenza, and solid tumor cancers. Females tend to experience more adverse reactions than males following the use of a class of biologics referred to as immunotherapies. For immunotherapies aimed at stimulating an immune response, e.g., influenza vaccines, females develop greater responses and may experience greater efficacy than males. In contrast, for immunotherapies that repress an immune response, e.g., tumor necrosis factor (TNF) inhibitors for RA or checkpoint inhibitors for melanoma, the efficacy is reportedly greater for males than females. Despite these differences, discrepancies in reporting differences between females and males exist, with females have been historically excluded from biomedical and clinical studies. There is a critical need for research that addresses the biological (i.e., sex) as well as sociocultural (i.e., gender) causes of male-female disparities in immunotherapy responses, toxicities, and outcomes. One-size-fits-all approaches to immunotherapies will not work, and sex/gender may contribute to variable treatment success, including adherence, in clinical settings.
Keywords: Autoimmunity; CTLA-4; Cancer; Checkpoint therapy; Influenza vaccine; PD-1/PD-L1; Rheumatoid arthritis; Tumor necrosis factor (TNF) inhibitor.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Wizemann TM, Pardue, M. (ed.): Exploring the biological contributions to human health: does sex matter? Washington DC: National Academy Press; 2001. - PubMed
-
- Guidelines FG: General considerations for the clinical evaluation of drugs. In.; 1977.
-
- Parekh A, Fadiran EO, Uhl K, Throckmorton DC. Adverse effects in women: implications for drug development and regulatory policies. Expert review of clinical pharmacology. 2011;4(4):453–466. - PubMed
-
- Pinn VW. The role of the NIH's office of research on women's health. Academic medicine : journal of the Association of American Medical Colleges. 1994;69(9):698–702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
