

Nosocomial outbreak of COVID-19 pneumonia in Wuhan, China
- PMID: 32366488
- PMCID: PMC7236818
- DOI: 10.1183/13993003.00544-2020
Nosocomial outbreak of COVID-19 pneumonia in Wuhan, China
Abstract
Background: The novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), infected over 3300 healthcare workers in early 2020 in China. Little information is known about nosocomial infections of healthcare workers in the initial period. We analysed data from healthcare workers with nosocomial infections in Wuhan Union Hospital (Wuhan, China) and their family members.
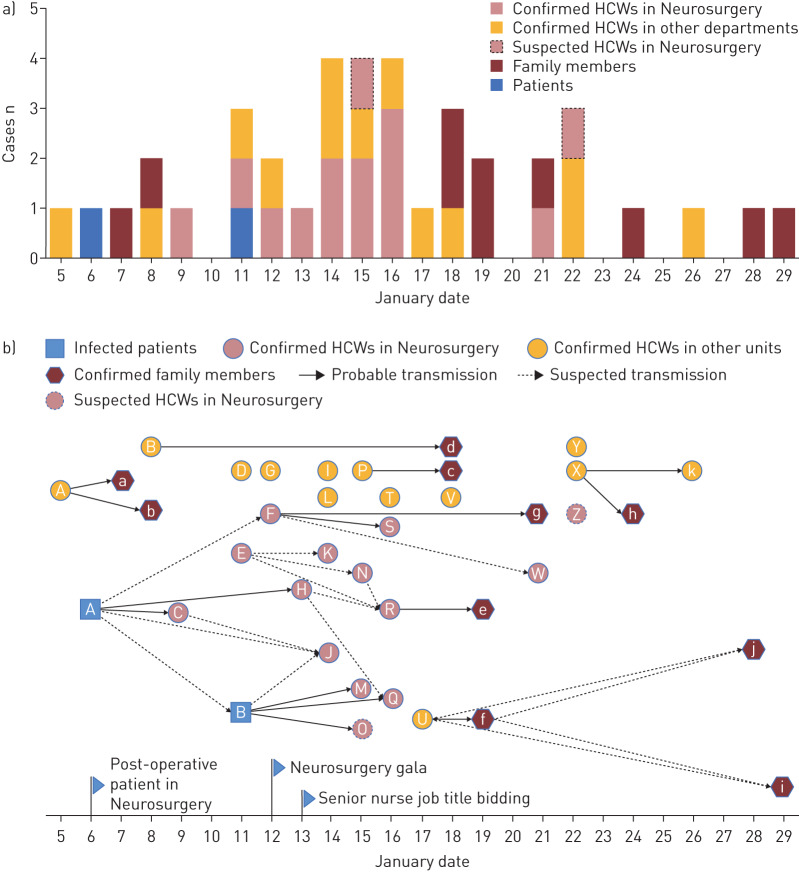
Methods: We collected and analysed data on exposure history, illness timelines and epidemiological characteristics from 25 healthcare workers with laboratory-confirmed coronavirus disease 2019 (COVID-19) and two healthcare workers in whom COVID-19 was highly suspected, as well as 10 of their family members with COVID-19, between 5 January and 12 February 2020. The demographics and clinical features of the 35 laboratory-confirmed cases were investigated and viral RNA of 12 cases was sequenced and analysed.
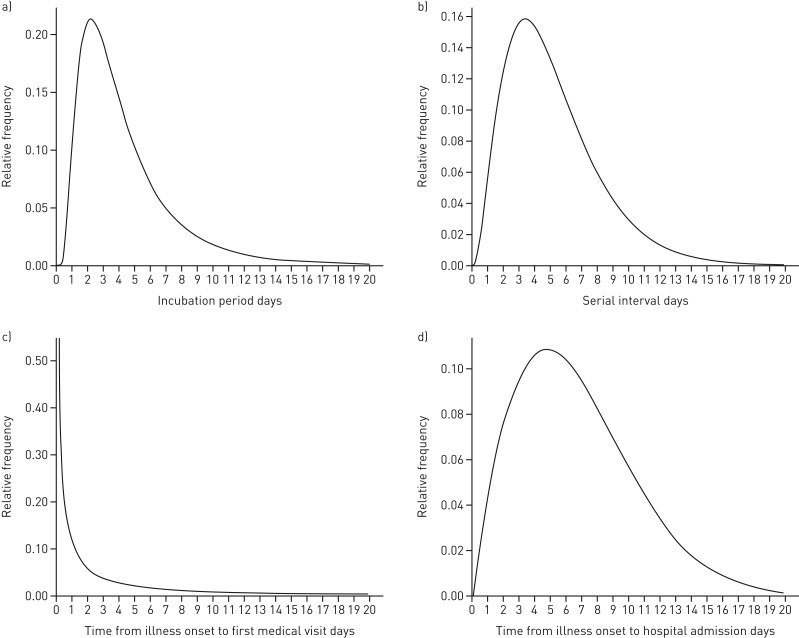
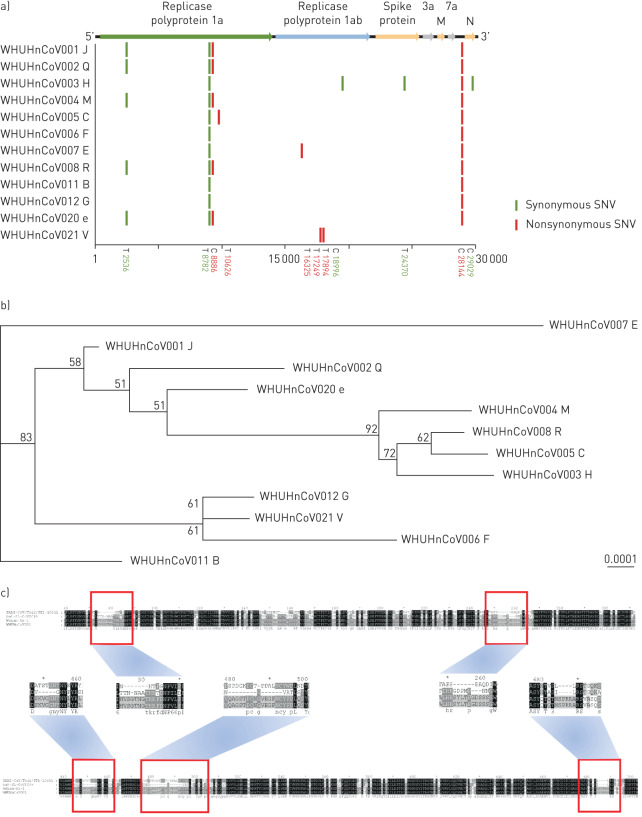
Results: Nine clusters were found among the patients. All patients showed mild to moderate clinical manifestation and recovered without deterioration. The mean period of incubation was 4.5 days, the mean±sd clinical onset serial interval (COSI) was 5.2±3.2 days, and the median virus shedding time was 18.5 days. Complete genomic sequences of 12 different coronavirus strains demonstrated that the viral structure, with small irrelevant mutations, was stable in the transmission chains and showed remarkable traits of infectious traceability.
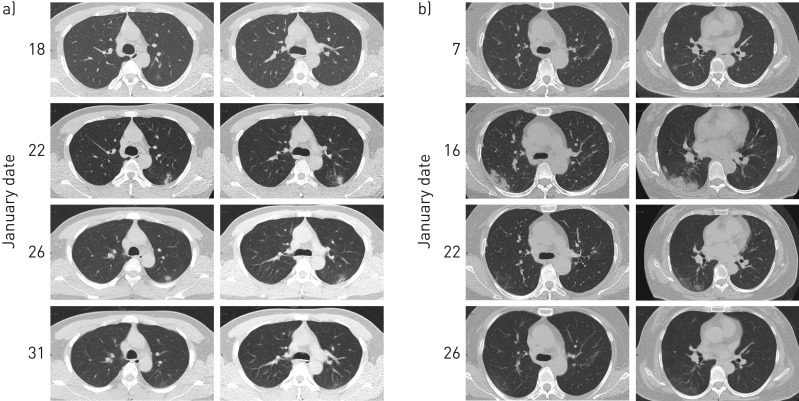
Conclusions: SARS-CoV-2 can be rapidly transmitted from person to person, regardless of whether they have symptoms, in both hospital settings and social activities, based on the short period of incubation and COSI. The public health service should take practical measures to curb the spread, including isolation of cases, tracing close contacts, and containment of severe epidemic areas. Besides this, healthcare workers should be alert during the epidemic and self-quarantine if self-suspected of infection.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: X. Wang has nothing to disclose. Conflict of interest: Q. Zhou has nothing to disclose. Conflict of interest: Y. He has nothing to disclose. Conflict of interest: L. Liu has nothing to disclose. Conflict of interest: X. Ma has nothing to disclose. Conflict of interest: X. Wei has nothing to disclose. Conflict of interest: N. Jiang has nothing to disclose. Conflict of interest: L. Liang has nothing to disclose. Conflict of interest: Y. Zheng has nothing to disclose. Conflict of interest: L. Ma has nothing to disclose. Conflict of interest: Y. Xu has nothing to disclose. Conflict of interest: D. Yang has nothing to disclose. Conflict of interest: J. Zhang has nothing to disclose. Conflict of interest: B. Yang has nothing to disclose. Conflict of interest: N. Jiang has nothing to disclose. Conflict of interest: T. Deng has nothing to disclose. Conflict of interest: B. Zhai has nothing to disclose. Conflict of interest: Y. Gao has nothing to disclose. Conflict of interest: W. Liu has nothing to disclose. Conflict of interest: X. Bai has nothing to disclose. Conflict of interest: T. Pan has nothing to disclose. Conflict of interest: G. Wang has nothing to disclose. Conflict of interest: Y. Chang has nothing to disclose. Conflict of interest: Z. Zhang has nothing to disclose. Conflict of interest: H. Shi has nothing to disclose. Conflict of interest: W-L. Ma has nothing to disclose. Conflict of interest: Z. Gao has nothing to disclose.
Figures
References
-
- National Health Commission of the People's Republic of China Update on new coronavirus pneumonia epidemic as of 24:00 on April 7. www.nhc.gov.cn/xcs/yqfkdt/202004/5e2b6f0bd47d48559582242e3878447d.shtml Date last updated: 8 April 2020. Date last accessed: 8 April 2020.
-
- Johns Hopkins University Center for Systems Science and Engineering COVID-19 global cases. https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594... Date last accessed: 8 April 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous