

Risk of first and recurrent serious infection in sarcoidosis: a Swedish register-based cohort study
- PMID: 32366492
- PMCID: PMC7469972
- DOI: 10.1183/13993003.00767-2020
Risk of first and recurrent serious infection in sarcoidosis: a Swedish register-based cohort study
Abstract
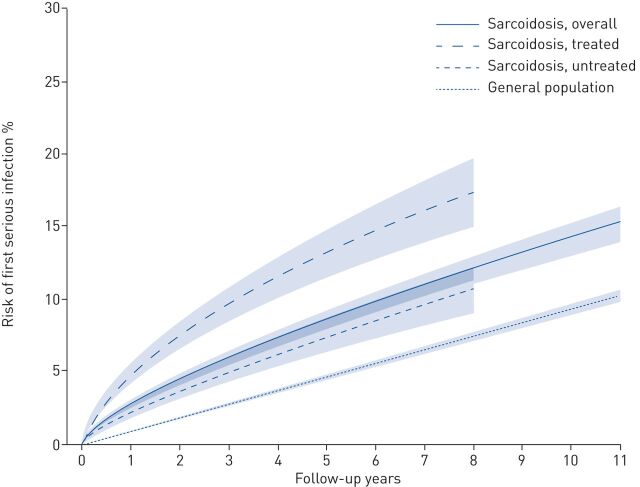
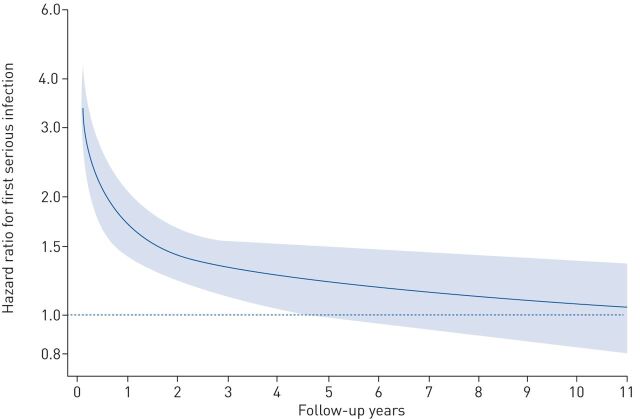
Serious infections impair quality of life and increase costs. Our aim was to determine if sarcoidosis is associated with a higher rate of serious infection and whether this varies by age, sex, time since diagnosis or treatment status around diagnosis.We compared individuals with sarcoidosis (at least two International Classification of Diseases codes in the Swedish National Patient Register 2003-2013; n=8737) and general population comparators matched 10:1 on age, sex and residential location (n=86 376). Patients diagnosed in 2006-2013 who were dispensed at least one immunosuppressant ±3 months from diagnosis (Swedish Prescribed Drug Register) were identified. Cases and comparators were followed in the National Patient Register for hospitalisations for infection. Using Cox and flexible parametric models, we estimated adjusted hazard ratios (aHR) and 95% confidence intervals for first and recurrent serious infections (new serious infection >30 days after previous).We identified 895 first serious infections in sarcoidosis patients and 3881 in comparators. The rate of serious infection was increased 1.8-fold in sarcoidosis compared to the general population (aHR 1.81, 95% CI 1.65-1.98). The aHR was higher in females than males and during the first 2 years of follow-up. Sarcoidosis cases treated with immunosuppressants around diagnosis had a three-fold increased risk, whereas nontreated patients had a 50% increased risk. The rate of serious infection recurrence was 2.8-fold higher in cases than in comparators.Serious infections are more common in sarcoidosis than in the general population, particularly during the first few years after diagnosis. Patients who need immunosuppressant treatment around diagnosis are twice as likely to develop a serious infection than those who do not.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: M. Rossides has nothing to disclose. Conflict of interest: S. Kullberg has nothing to disclose. Conflict of interest: A. Eklund has nothing to disclose. Conflict of interest: D. Di Giuseppe has nothing to disclose. Conflict of interest: J. Grunewald reports grants from Swedish Heart-Lung Foundation (Hjärt-Lungfonden; grant number 20190478), during the conduct of the study. Conflict of interest: J. Askling has nothing to disclose. Conflict of interest: E.V. Arkema reports grants from Swedish Heart-Lung Foundation (Hjärt-Lungfonden; grant number 20170412), during the conduct of the study. Conflict of interest: M. Rossides has nothing to disclose.
Figures
Comment in
-
Sarcoidosis in a time of pandemic.Eur Respir J. 2020 Sep 3;56(3):2002376. doi: 10.1183/13993003.02376-2020. Print 2020 Sep. Eur Respir J. 2020. PMID: 32883761 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical