

Glucocorticoid-Induced Fatty Liver Disease
- PMID: 32368109
- PMCID: PMC7171875
- DOI: 10.2147/DMSO.S247379
Glucocorticoid-Induced Fatty Liver Disease
Abstract
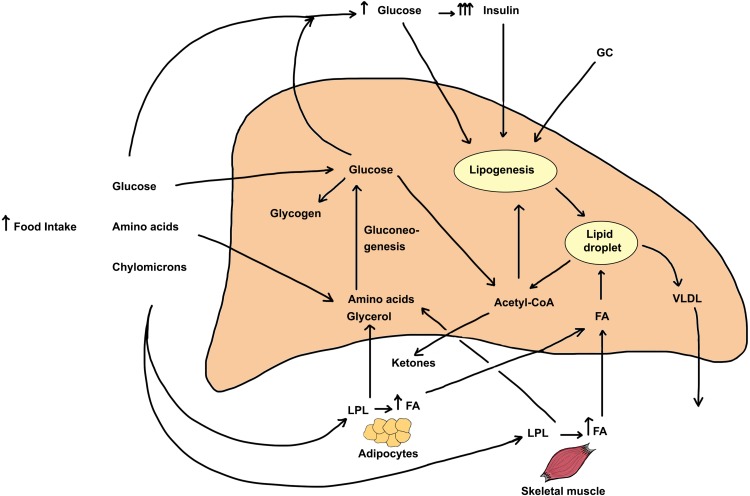
Glucocorticoids (GCs) are commonly used at high doses and for prolonged periods (weeks to months) in the treatment of a variety of diseases. Among the many side effects are increased insulin resistance with disturbances in glucose/insulin homeostasis and increased deposition of lipids (mostly triglycerides) in the liver. Here, we review the metabolic pathways of lipid deposition and removal from the liver that become altered by excess glucocorticoids. Pathways of lipid deposition stimulated by excess glucocorticoids include 1) increase in appetite and high caloric intake; 2) increased blood glucose levels due to GC-induced stimulation of gluconeogenesis; 3) stimulation of de novo lipogenesis that is augmented by the high glucose and insulin levels and by GC itself; and 4) increased release of free fatty acids from adipose stores and stimulation of their uptake by the liver. Pathways that decrease hepatic lipids affected by glucocorticoids include a modest stimulation of very-low-density lipoprotein synthesis and secretion into the circulation and inhibition of β-oxidation of fatty acids. Role of 11β-hydroxysteroid dehydrogenases-1 and -2 and the reversible conversion of cortisol to cortisone on intracellular levels of cortisol is examined. In addition, GC control of osteocalcin expression and the effect of this bone-derived hormone in increasing insulin sensitivity are discussed. Finally, research focused on gaining a better understanding of the dose and duration of treatment with glucocorticoids, which leads to increased triglyceride deposition in the liver, and the reversibility of the condition is highlighted.
Keywords: Cushing’s disease; LPL; fatty liver; hormone-sensitive lipase; hyperphagia; metabolic syndrome; obesity.
© 2020 Rahimi et al.
Conflict of interest statement
Faramarz Ismail-Beigi is a consultant for Sanofi and COVANCE. He has grants from the NIH, and has previously received grants from Novo Nordisk; he has shares in Thermalin Insulin. The authors report no other conflicts of interest in this work.
Figures
References
-
- Marino JS, Stechschulte LA, Stec DE, Nestor-Kalinoski A, Coleman S, Hinds TD Jr. Glucocorticoid receptor β induces hepatic steatosis by augmenting inflammation and inhibition of the peroxisome proliferator-activated receptor (PPAR) α. J Biol Chem. 2016;291(50):25776–25788. doi:10.1074/jbc.M116.752311 - DOI - PMC - PubMed
-
- Der Laan SV, Onno C, Meijer OC. Pharmacology of glucocorticoids: beyond receptors. Eur J Pharmcol. 2008;585:3483–3491. - PubMed
-
- Shibli-Rahhal A, Van Beek M, Schlechte JA. Cushing’s syndrome. Clin Dermatol. 2006;24(4):260–265. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
