

Temporal trends of incident diabetes mellitus and subsequent outcomes in patients receiving kidney transplantation: a national cohort study in Taiwan
- PMID: 32368254
- PMCID: PMC7189729
- DOI: 10.1186/s13098-020-00541-3
Temporal trends of incident diabetes mellitus and subsequent outcomes in patients receiving kidney transplantation: a national cohort study in Taiwan
Abstract
Background: Allograft kidney transplantation has become a treatment of choice for patients with end-stage renal disease (ESRD), and post-transplant diabetes mellitus (PTDM) has been associated with impaired patient and graft survival. Taiwan has the highest incidence and prevalence rates of ESRD with many recipients and candidates of kidney transplantation. However, information about the epidemiologic features of PTDM in Taiwan is incomplete. Therefore, we aimed to investigate the prevalence and incidence of PTDM with subsequent patient and graft outcomes.
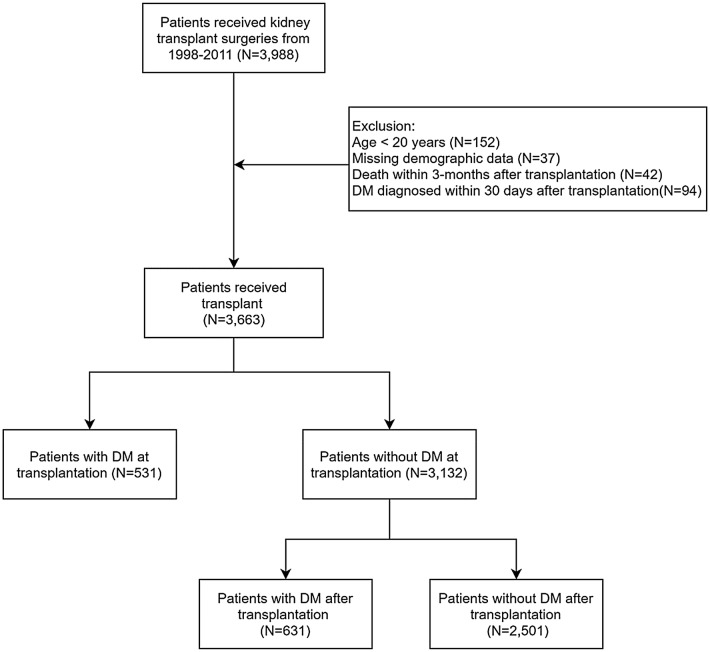
Methods: Using the Taiwan National Health Insurance Research Database (NHIRD), 3663 kidney recipients between 1997 and 2011 were enrolled. We calculated the cumulative incidences of diabetes mellitus (DM) after transplantation. Cox proportional hazards model with competing risk analysis was used to calculate the hazard ratio (HR) and 95% confidence intervals (CI) between three targeted groups (DM, PTDM, non-DM). The outcomes of primary interest were the occurrence of graft failure excluding death with functioning graft, all-cause mortality, death with functioning graft and major adverse cardiovascular events (MACE) including myocardial infarction (MI), cerebrovascular accident (CVA) and congestive heart failure (CHF). Subgroup analysis for graft failure excluding death with functioning graft, MACE and all-cause mortality was performed, and interaction between PTDM and recipient age was examined.
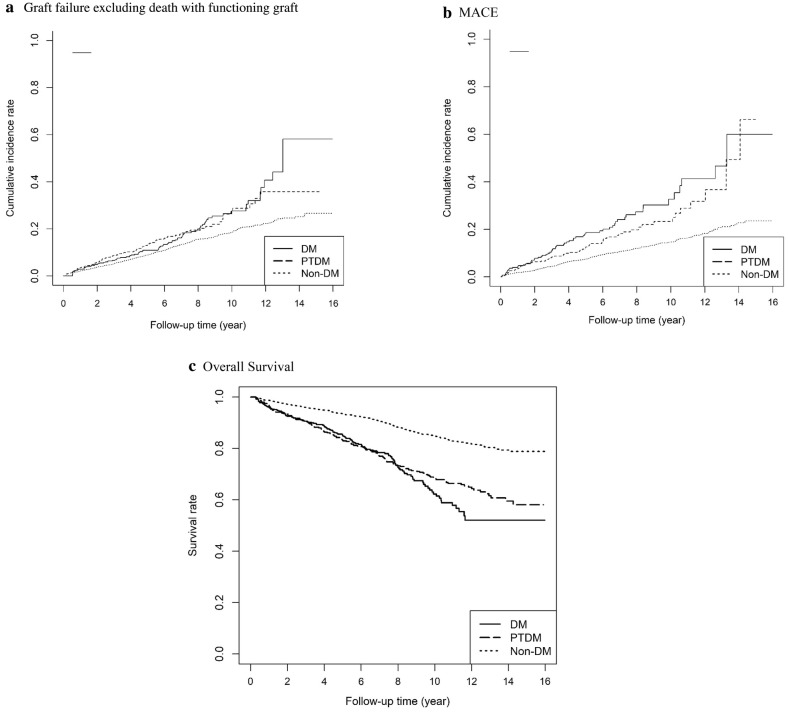
Results: Of 3663 kidney transplant recipients, 531 (14%) had pre-existing DM and 631 (17%) developed PTDM. Compared with non-DM group, the PTDM and DM groups exhibited higher risk of graft failure excluding death with functioning graft (PTDM: HR 1.65, 95% CI 1.47-1.85; DM: HR 1.33, 95% CI 1.18-1.50), MACE (PTDM: HR 1.51, 95% CI 1.31-1.74; DM: HR 1.64, 95% CI 1.41-1.9), all-cause mortality (PTDM: HR 1.79, 95% CI 1.59-2.01; DM: HR 2.03, 95% CI 1.81-2.18), and death with functioning graft (PTDM: HR 1.94, 95% CI 1.71-2.20; DM: HR 1.94, 95% CI 1.71-2.21). Both PTDM and DM groups had increased cardiovascular disease-related mortality (PTDM: HR 2.14, 95% CI 1.43-3.20, p < 0.001; DM: HR 1.89, 95% CI 1.25-2.86, p = 0.002), cancer-related mortality (PTDM: HR 1.56, 95% CI 1.18-2.07, p = 0.002; DM: HR 1.89, 95% CI 1.25-2.86, p = 0.027), and infection-related mortality (PTDM: HR 1.47, 95% CI 1.14-1.90, p = 0.003; DM: HR 2.25, 95% CI 1.77-2.84, p < 0.001) compared with non-DM group. The subgroup analyses showed that the add-on risks of MACE and mortality from PTDM were mainly observed in patients who were younger and those without associated comorbidities including atrial fibrillation, cirrhosis, CHF, and MI. Age significantly modified the association between PTDM and MACE (pinteraction < 0.01) with higher risk in recipients with PTDM aged younger than 55 years (adjusted HR 1.64, 95% CI 1.40-1.92, p < 0.001). A trend (pinteraction = 0.06) of age-modifying effect on the association between PTDM and all-cause mortality was also noted with higher risk in recipients with PTDM aged younger than 55 years.
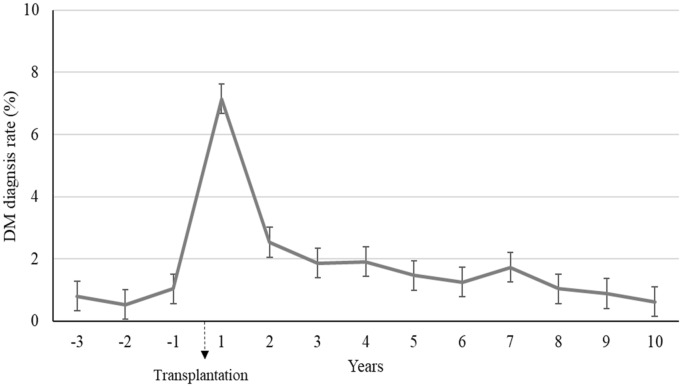
Conclusions: In the present population-based study, the incidence of PTDM peaked within the first year after kidney transplantation. PTDM negatively impacted graft and patient outcomes. The magnitude of cardiovascular and survival disadvantages from PTDM were more pronounced in recipients aged less than 55 years. Further trials to improve prediction of PTDM and to prevent PTDM are warranted.
Keywords: Graft failure; Kidney transplantation; Post-transplantation diabetic mellitus.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
LinkOut - more resources
Full Text Sources
