

Impact of checkpoint blockade on cancer vaccine-activated CD8+ T cell responses
- PMID: 32369107
- PMCID: PMC7336310
- DOI: 10.1084/jem.20191369
Impact of checkpoint blockade on cancer vaccine-activated CD8+ T cell responses
Abstract
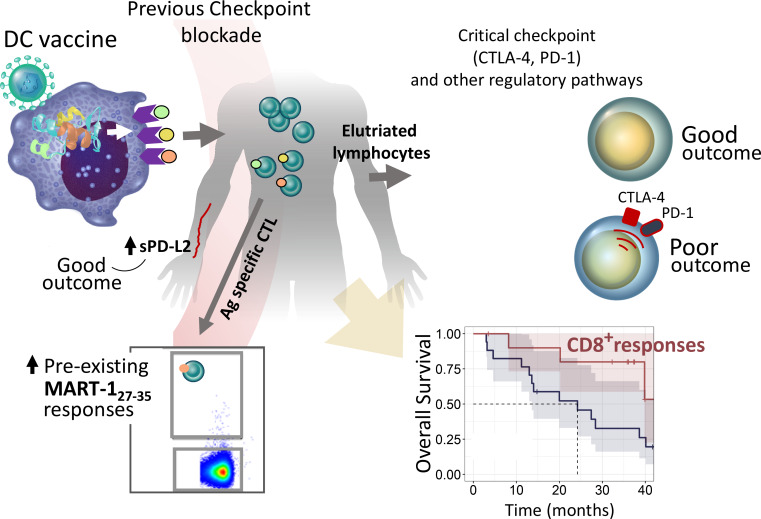
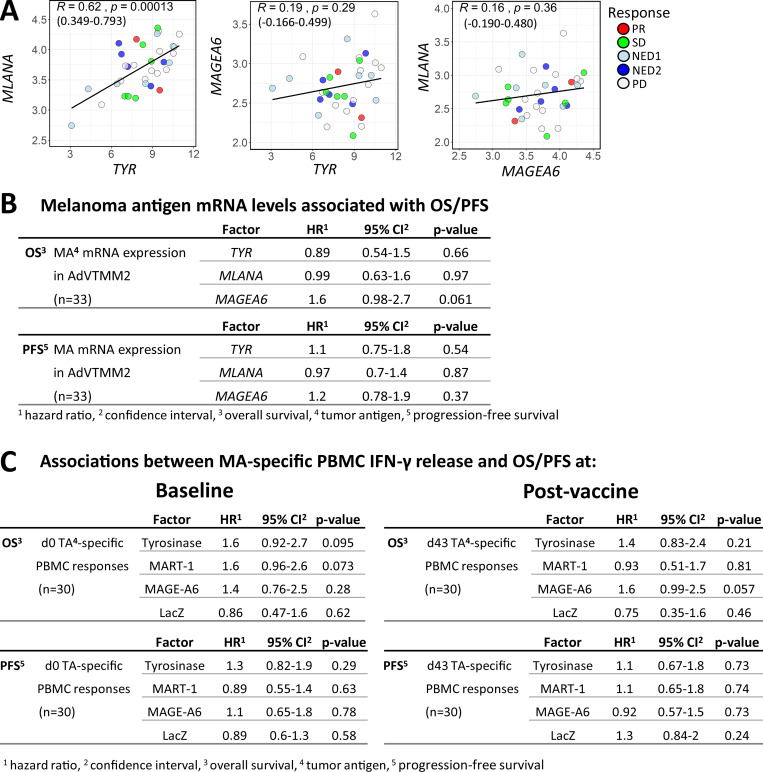
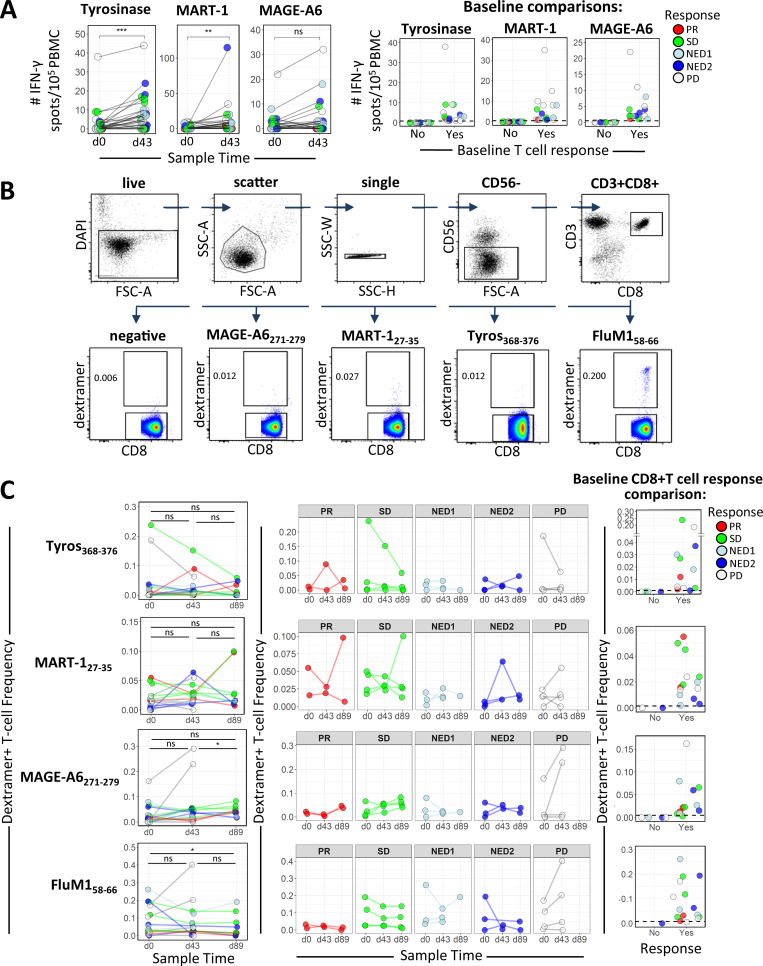
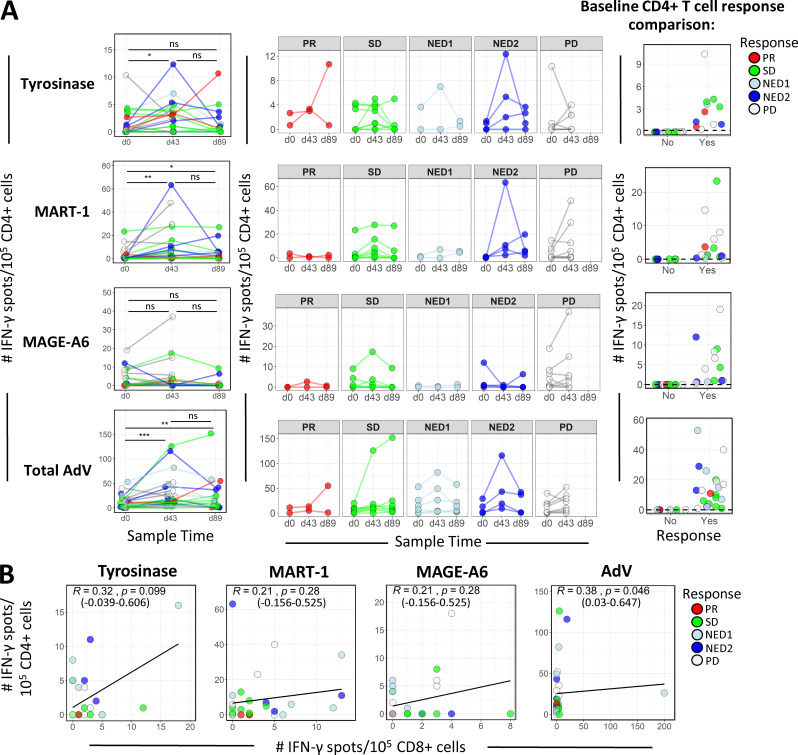
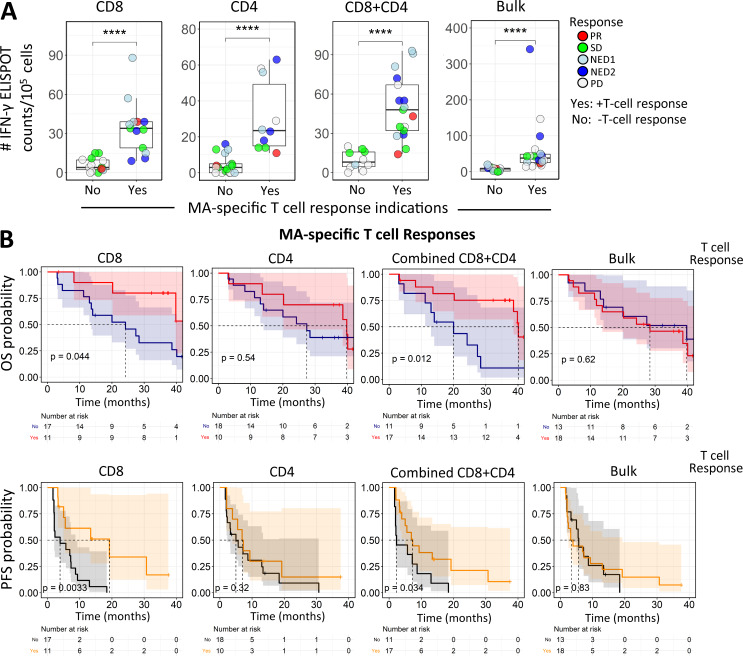
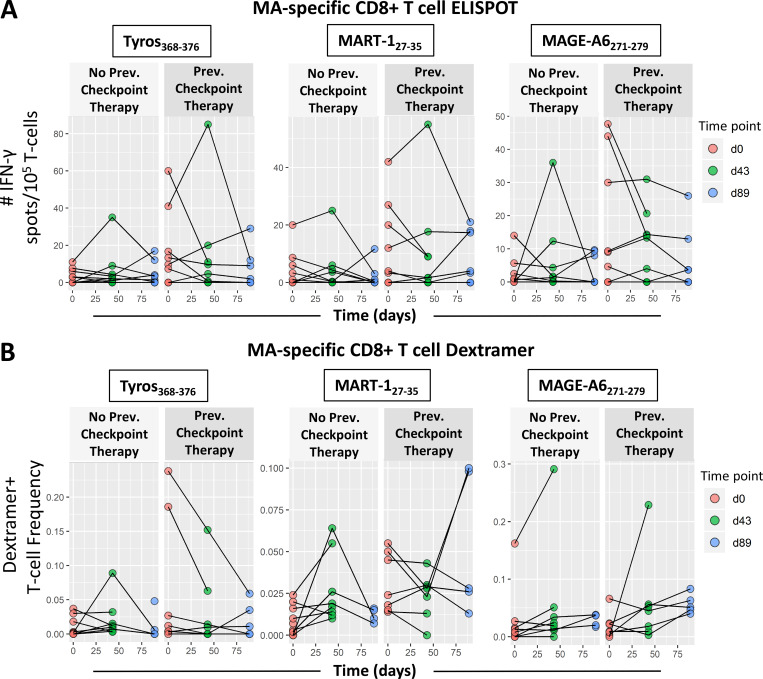
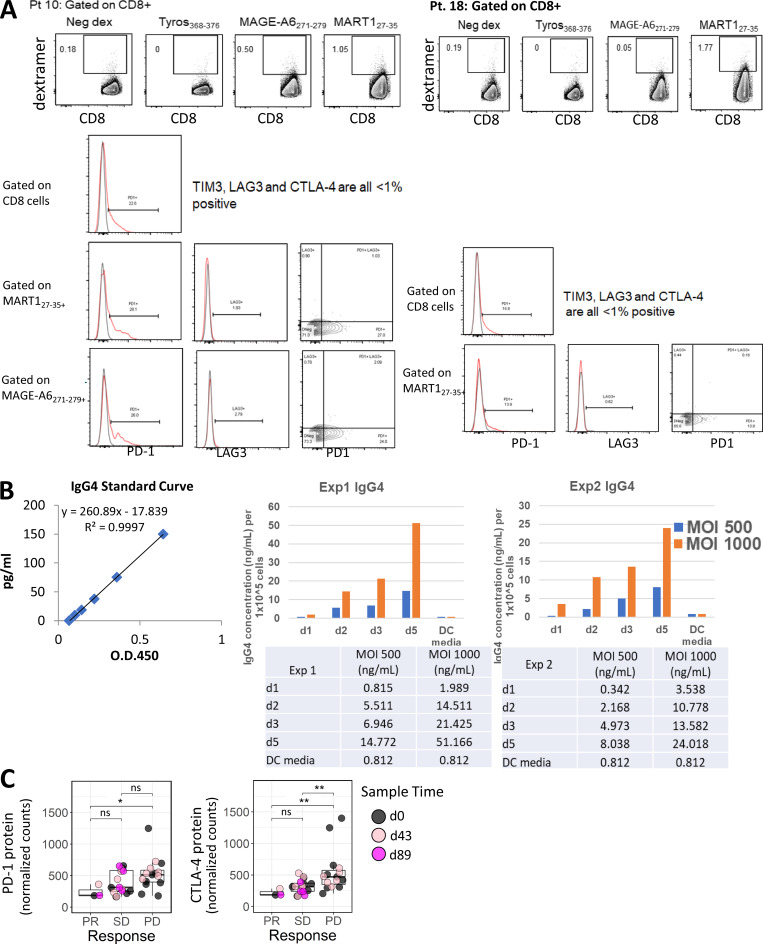
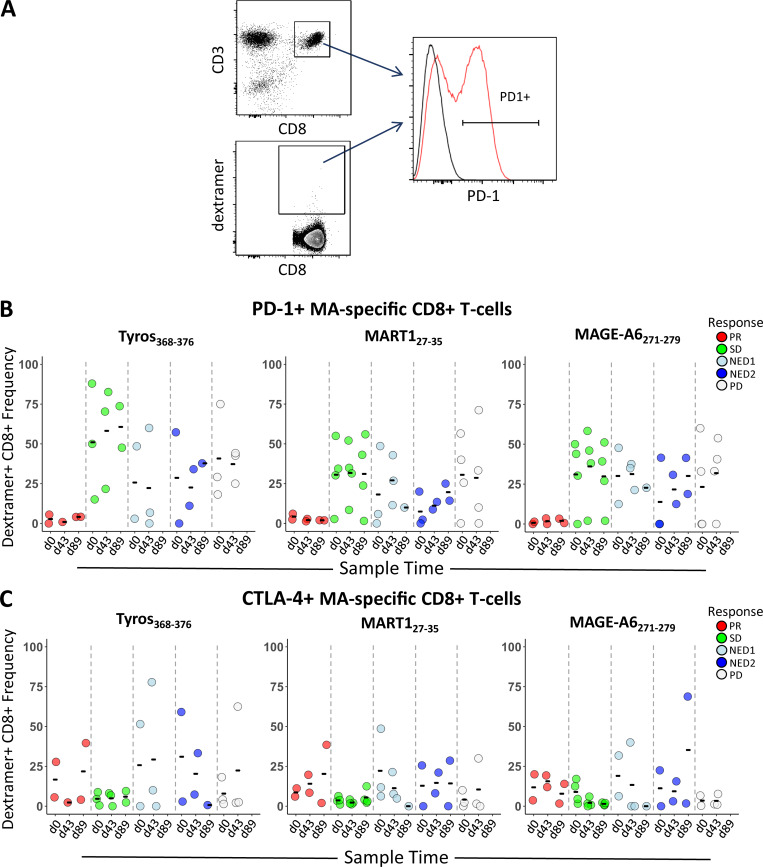
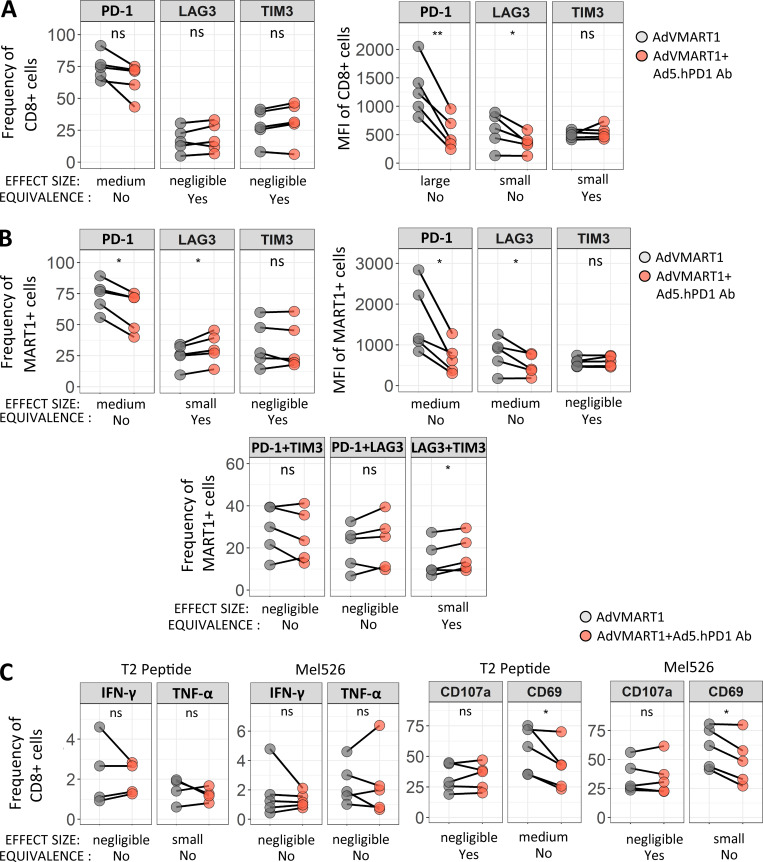
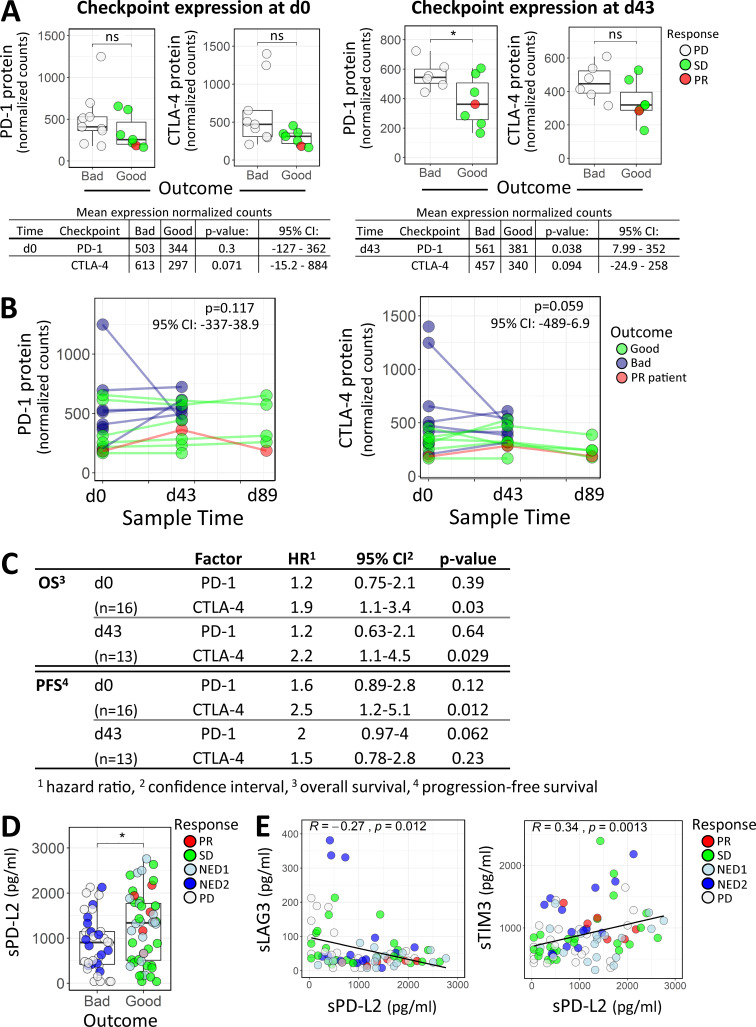
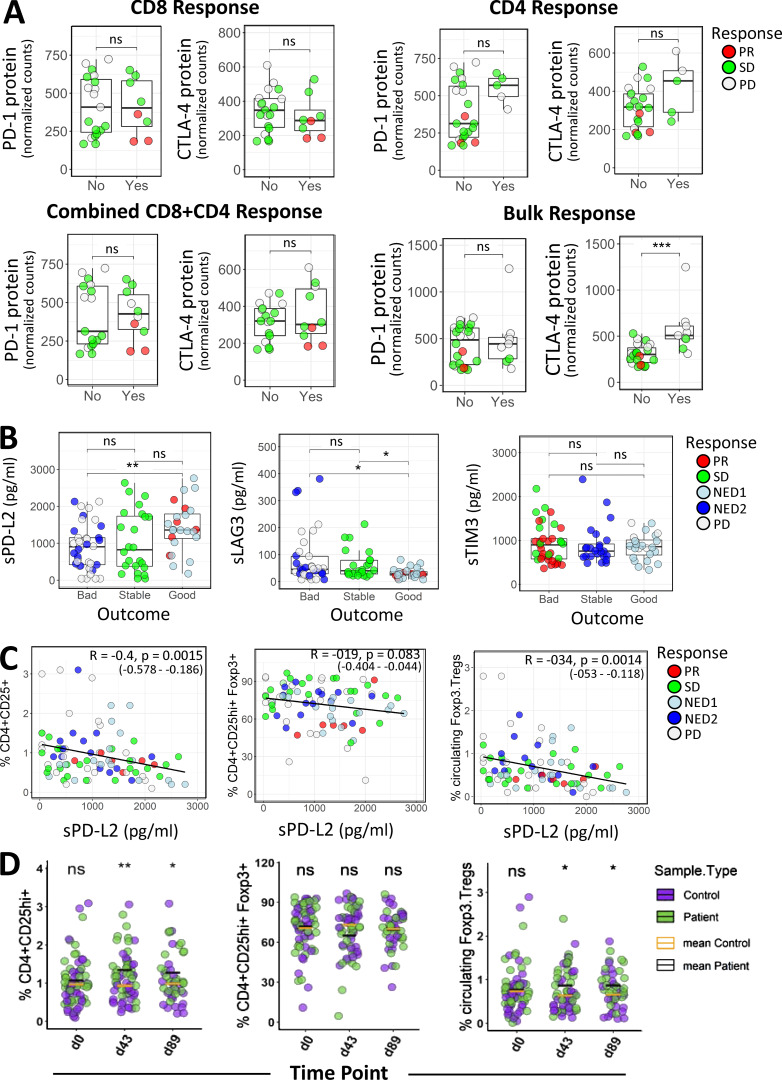
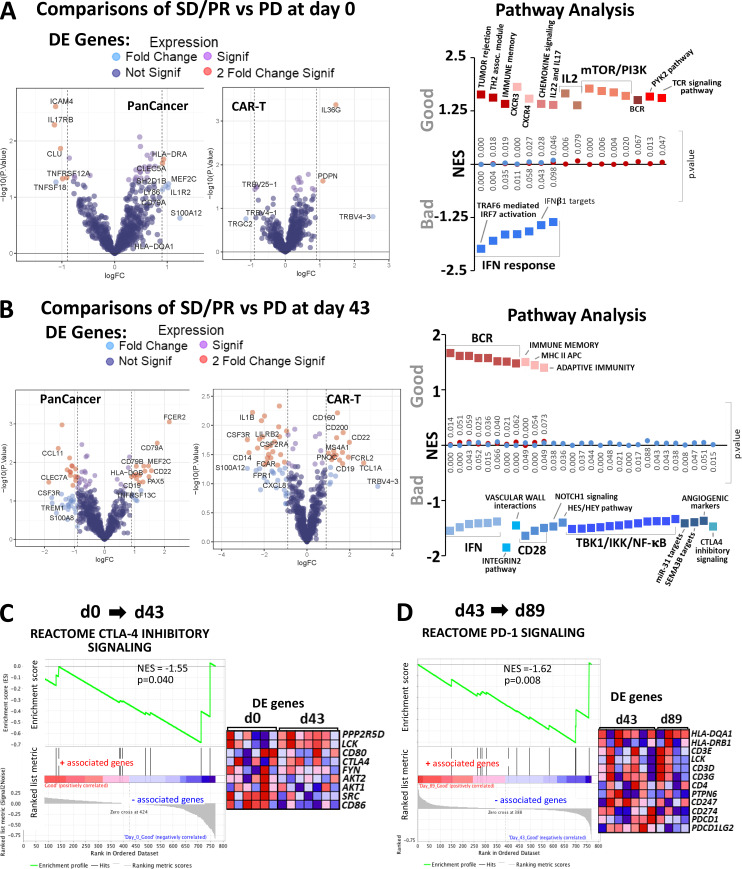
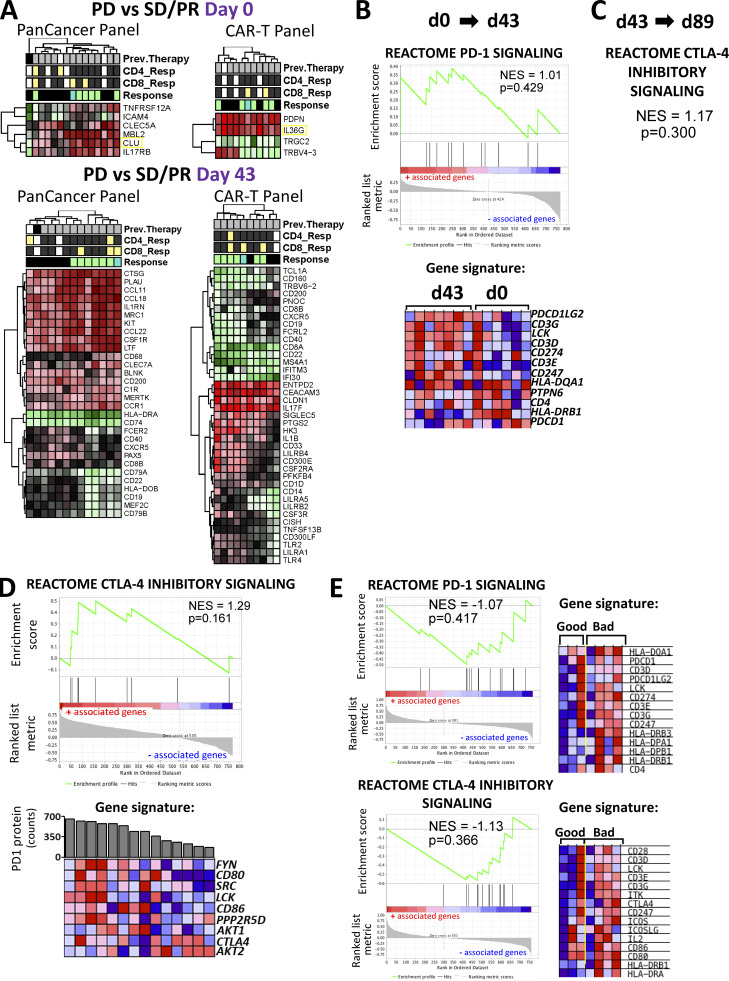
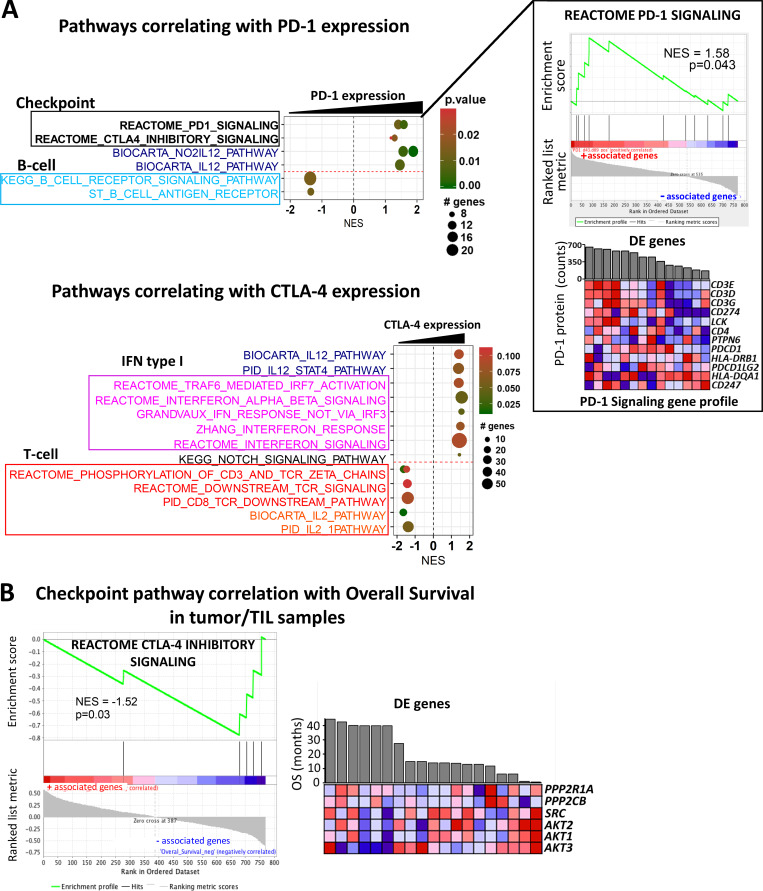
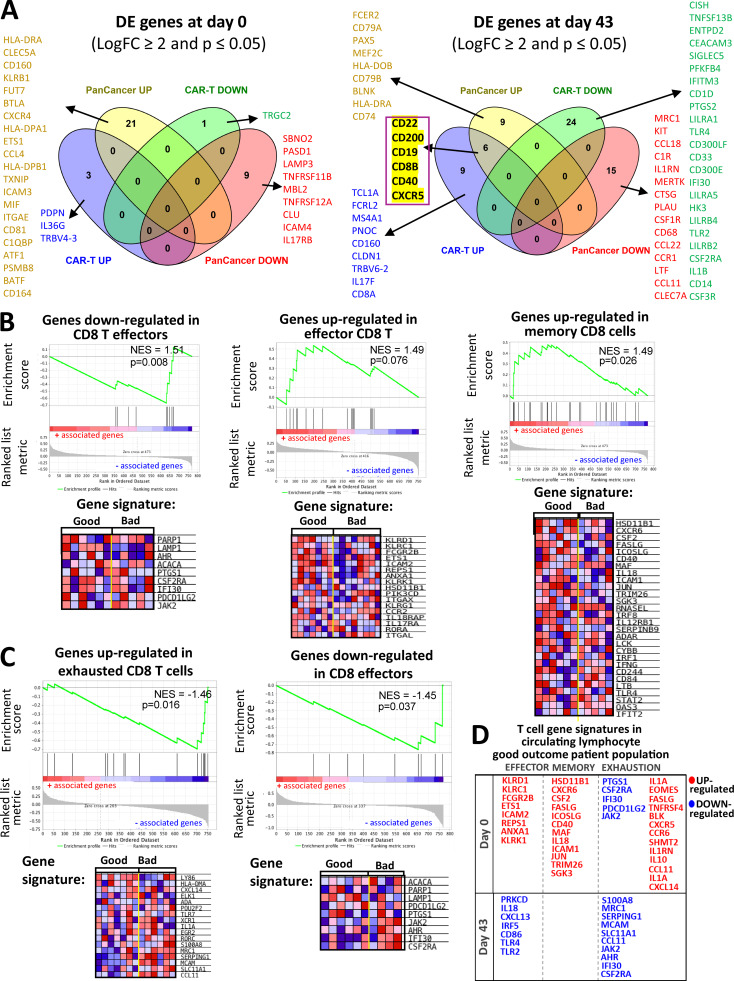
Immune and molecular profiling of CD8 T cells of patients receiving DC vaccines expressing three full-length melanoma antigens (MAs) was performed. Antigen expression levels in DCs had no significant impact on T cell or clinical responses. Patients who received checkpoint blockade before DC vaccination had higher baseline MA-specific CD8 T cell responses but no evidence for improved functional responses to the vaccine. Patients who showed the best clinical responses had low PD-1 expression on MA-specific T cells before and after DC vaccination; however, blockade of PD-1 during antigen presentation by DC had minimal functional impact on PD-1high MA-specific T cells. Gene and protein expression analyses in lymphocytes and tumor samples identified critical immunoregulatory pathways, including CTLA-4 and PD-1. High immune checkpoint gene expression networks correlated with inferior clinical outcomes. Soluble serum PD-L2 showed suggestive positive association with improved outcome. These findings show that checkpoint molecular pathways are critical for vaccine outcomes and suggest specific sequencing of vaccine combinations.
© 2020 Santos et al.
Conflict of interest statement
Disclosures: Dr. Warren reported personal fees from Nanostring Technology during the conduct of the study. Dr. Kirkwood reported grants from Amgen, Inc., BMS, Castle Biosciences, Checkmate, Immunocore, Iovance, Merck, and Novartis; and personal fees from Amgen, Inc., BMS, Elsevier, Novartis, Iovance, and Immunocore, LLC, outside the submitted work. Dr. Butterfield reported personal fees from Calidi, SapVax, Replimmune, Western Oncolytics, Torque, Pyxis, NextCure, Vir, Cytomix, and Roche-Genentech outside the submitted work. No other disclosures were reported.
Figures
References
-
- Appleman L.J., Normolle D.P., Logan T.F., Monk P., Olencki T., McDermott D.F., Ernstoff M.S., Maranchie J.K., Parikh R.A., Friedland D., et al. . 2018. Safety and activity of hydroxychloroquine and aldesleukin in metastatic renal cell carcinoma: A cytokine working group phase II study. J. Clin. Oncol. 36(15_suppl):4573 10.1200/JCO.2018.36.15_suppl.4573 - DOI
-
- Benci J.L., Xu B., Qiu Y., Wu T.J., Dada H., Twyman-Saint Victor C., Cucolo L., Lee D.S.M., Pauken K.E., Huang A.C., et al. . 2016. Tumor Interferon Signaling Regulates a Multigenic Resistance Program to Immune Checkpoint Blockade. Cell. 167:1540–1554.e12. 10.1016/j.cell.2016.11.022 - DOI - PMC - PubMed
-
- Butterfield L.H., Jilani S.M., Chakraborty N.G., Bui L.A., Ribas A., Dissette V.B., Lau R., Gamradt S.C., Glaspy J.A., McBride W.H., et al. . 1998. Generation of melanoma-specific cytotoxic T lymphocytes by dendritic cells transduced with a MART-1 adenovirus. J. Immunol. 161:5607–5613. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
