

Tryptophan catabolism reflects disease activity in human tuberculosis
- PMID: 32369456
- PMCID: PMC7259525
- DOI: 10.1172/jci.insight.137131
Tryptophan catabolism reflects disease activity in human tuberculosis
Abstract
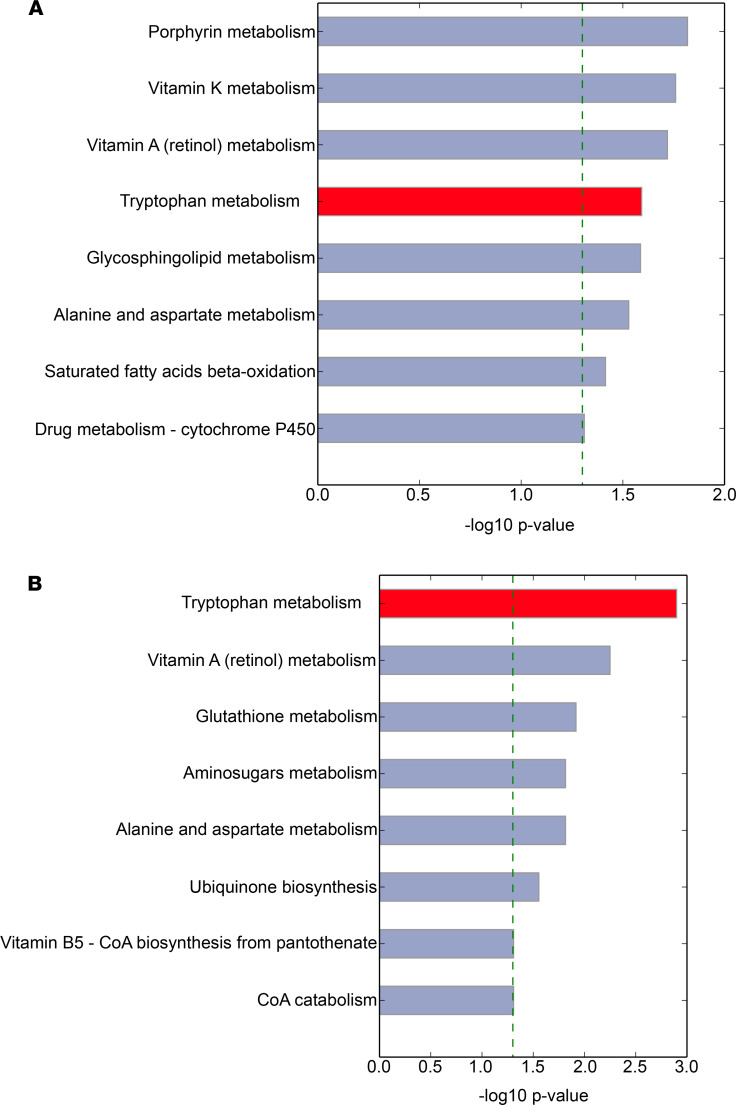
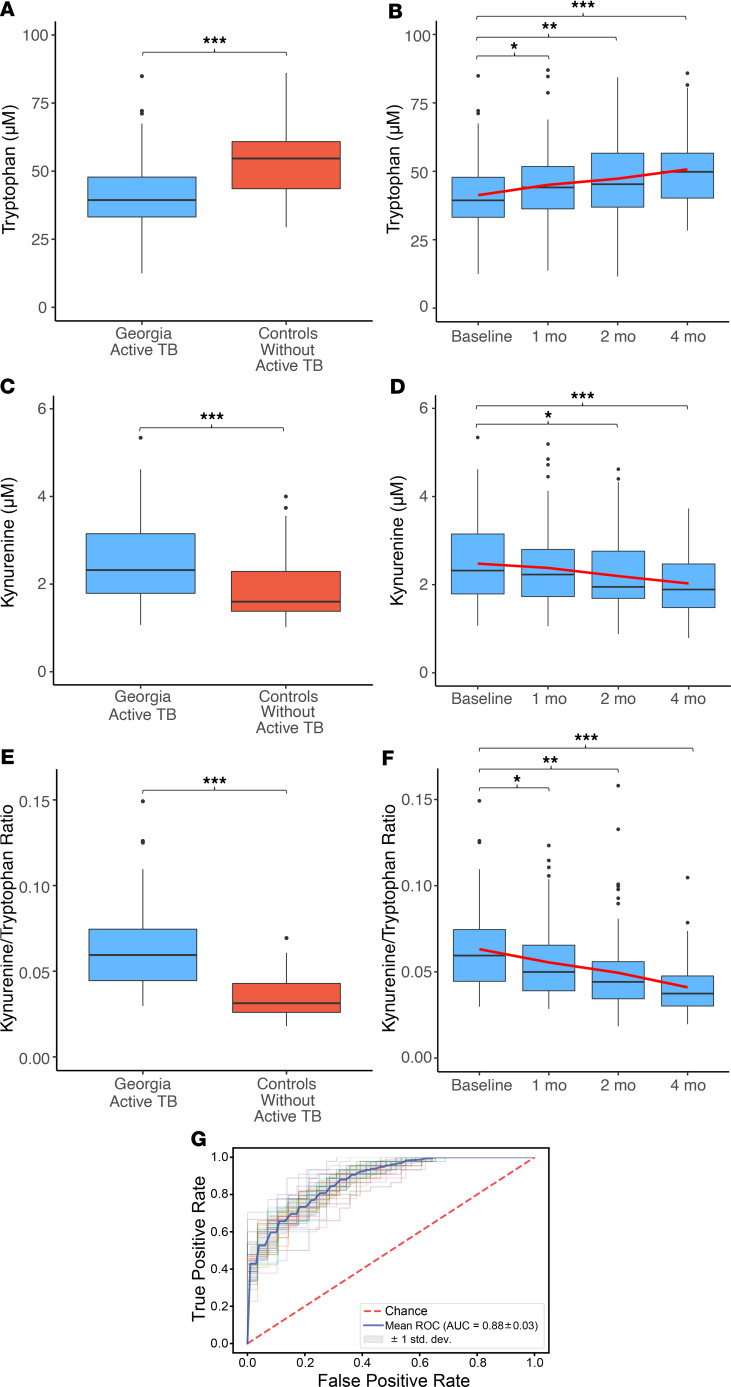
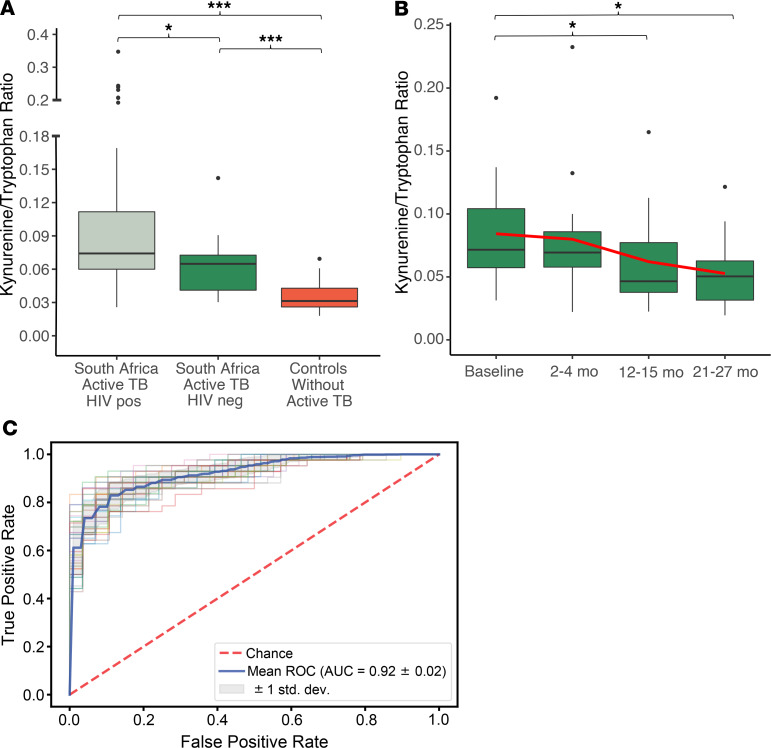
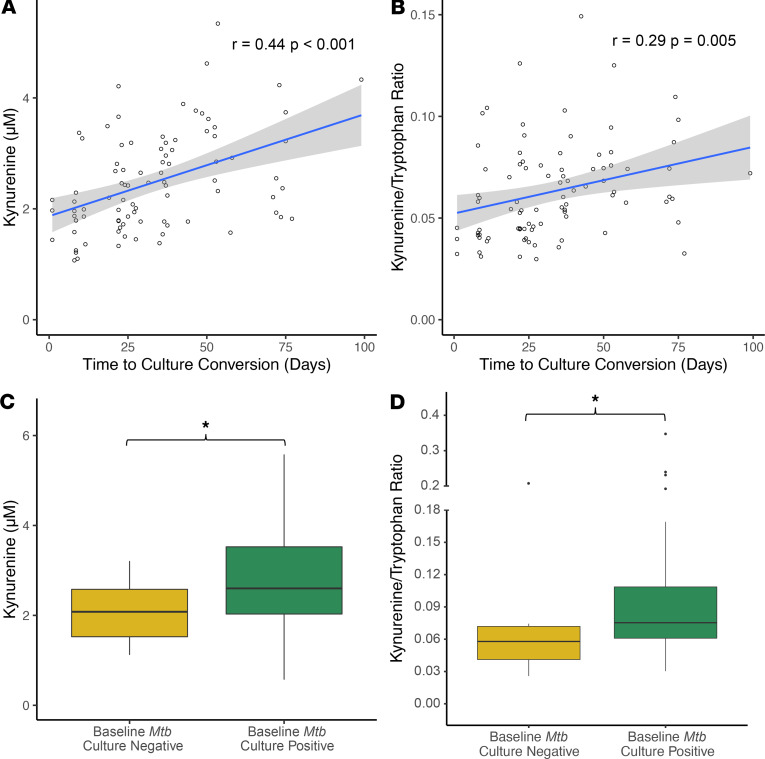
There is limited understanding of the role of host metabolism in the pathophysiology of human tuberculosis (TB). Using high-resolution metabolomics with an unbiased approach to metabolic pathway analysis, we discovered that the tryptophan pathway is highly regulated throughout the spectrum of TB infection and disease. This regulation is characterized by increased catabolism of tryptophan to kynurenine, which was evident not only in active TB disease but also in latent TB infection (LTBI). Further, we found that tryptophan catabolism is reversed with effective treatment of both active TB disease and LTBI in a manner commensurate with bacterial clearance. Persons with active TB and LTBI also exhibited increased expression of indoleamine 2,3-dioxygenase-1 (IDO-1), suggesting IDO-1 mediates observed increases in tryptophan catabolism. Together, these data indicate IDO-1-mediated tryptophan catabolism is highly preserved in the human response to Mycobacterium tuberculosis and could be a target for biomarker development as well as host-directed therapies.
Keywords: Infectious disease; Metabolism; Tuberculosis.
Conflict of interest statement
Figures


References
-
- WHO. World Health Organization Global Tuberculosis Report 2019. WHO. https://www.who.int/tb/publications/global_report/en/ Published October 17, 2019. Accessed April 30, 2020.
