

Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis
- PMID: 32370055
- PMCID: PMC7290699
- DOI: 10.3390/jcm9051305
Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis
Abstract
Background: Human papillomavirus (HPV) infection has been recognized as an important risk factor in cancer. The purpose of this systematic review and meta-analysis was to determine the prevalence and effect size of association between salivary HPV DNA and the risk of developing oral and oropharyngeal cancer.
Methods: A systematic literature search of PubMed, EMBASE, Web of Science, LILACS, Scopus and the Cochrane Library was performed, without language restrictions or specified start date. Pooled data were analyzed by calculating odds ratios (ORs) and 95% confidence intervals (CIs). Quality assessment was performed using the Newcastle-Ottawa Scale (NOS).
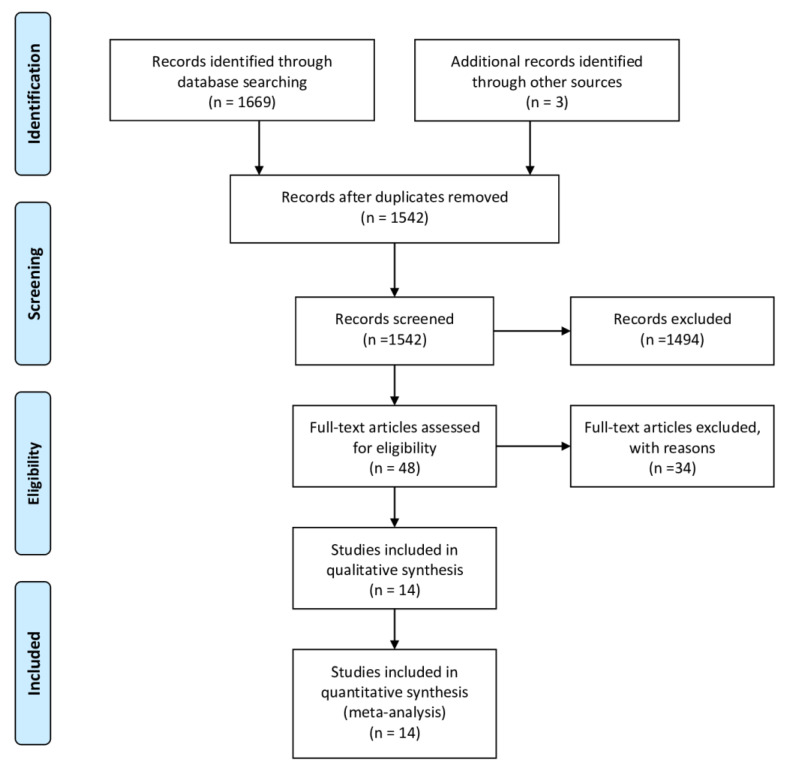
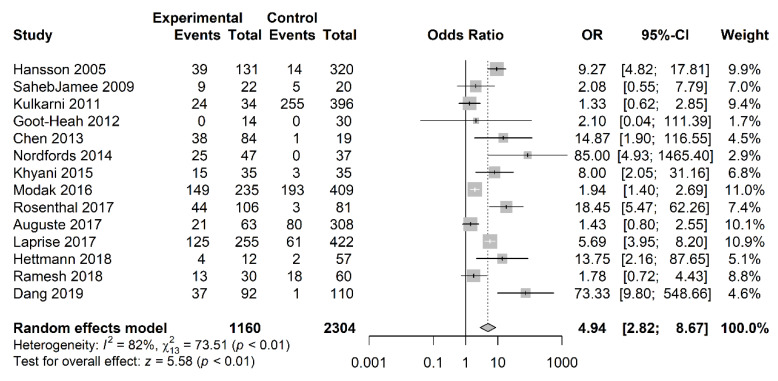
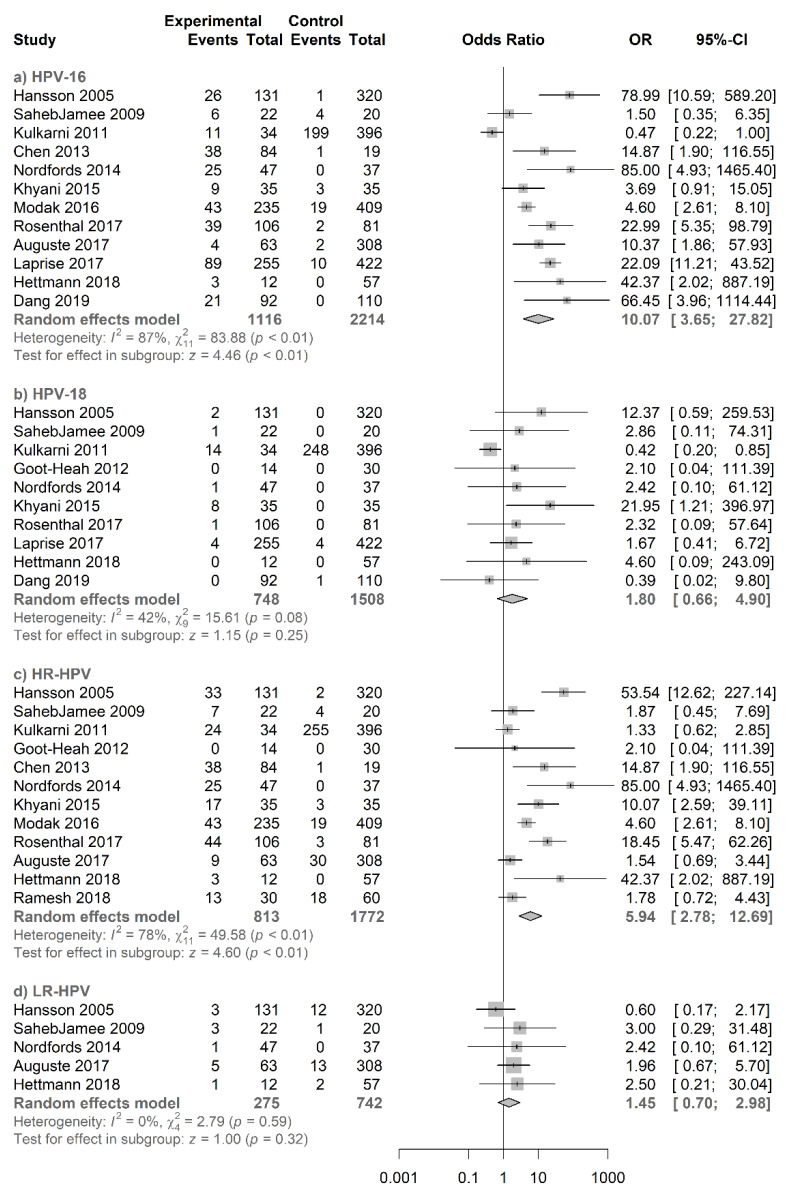
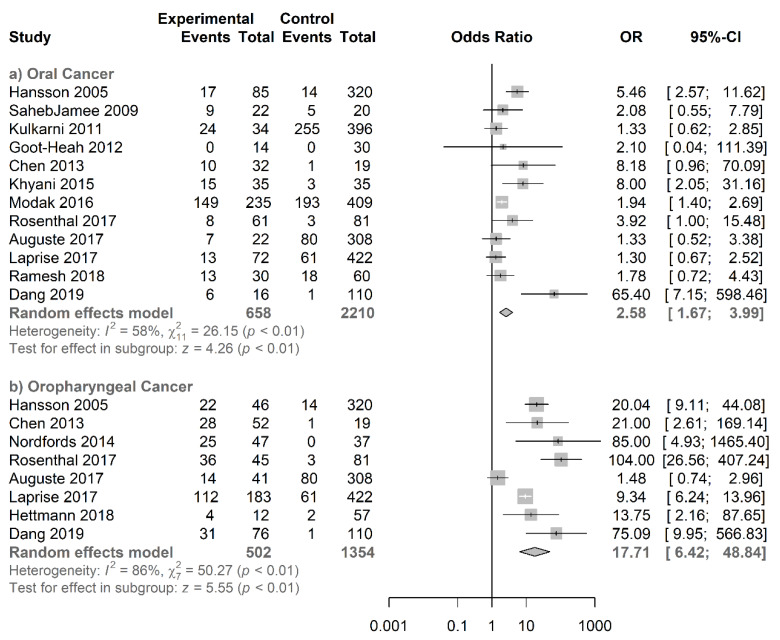
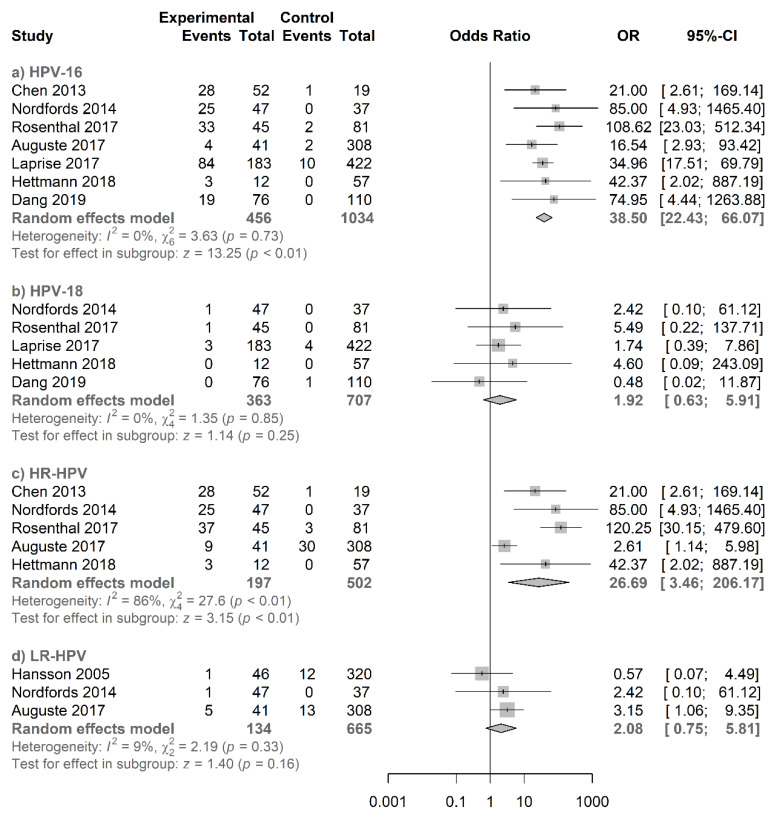
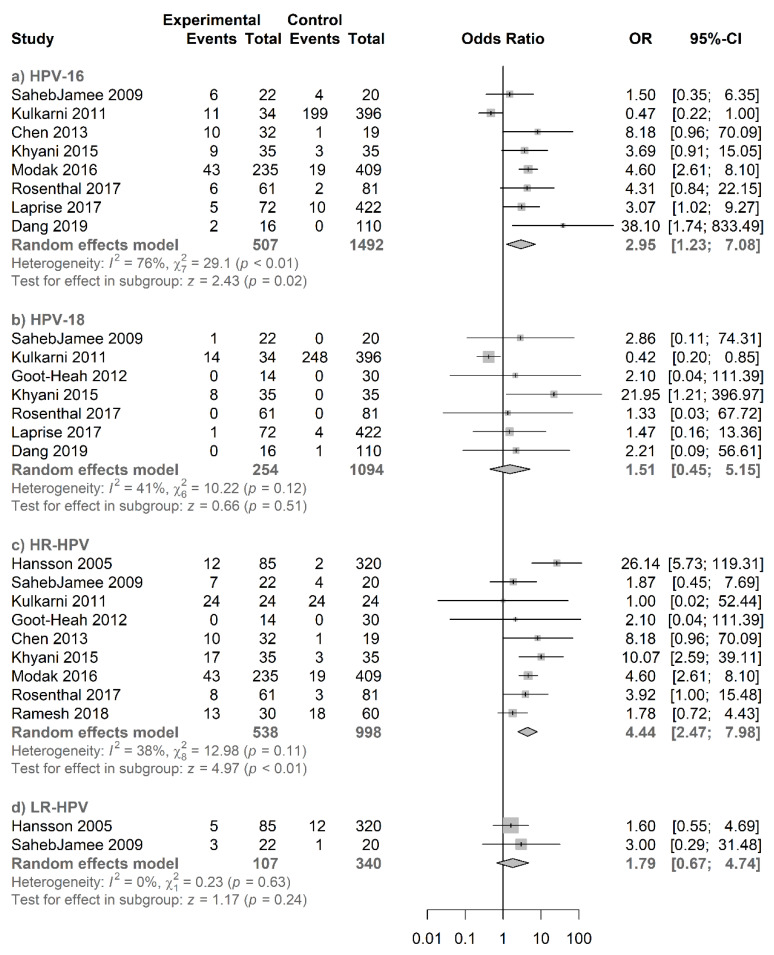
Results: A total of 1672 studies were screened and 14 met inclusion criteria for the meta-analysis. The overall prevalence of salivary HPV DNA for oral and oropharyngeal carcinoma was 43.2%, and the prevalence of salivary HPV16 genotype was 27.5%. Pooled results showed a significant association between salivary HPV and oral and oropharyngeal cancer (OR = 4.94; 2.82-8.67), oral cancer (OR = 2.58; 1.67-3.99) and oropharyngeal cancer (OR = 17.71; 6.42-48.84). Significant associations were also found between salivary HPV16 and oral and oropharyngeal cancer (OR = 10.07; 3.65-27.82), oral cancer (OR = 2.95; 1.23-7.08) and oropharyngeal cancer (OR = 38.50; 22.43-66.07).
Conclusions: Our meta-analysis demonstrated the association between salivary HPV infection and the incidence of oral and oropharyngeal cancer indicating its value as a predictive indicator.
Keywords: human papillomavirus; meta-analysis; oral cancer; oropharyngeal cancer; saliva.
Conflict of interest statement
R.L.-L. reports other from Nasasbiotech, during the conduct of the study; grants and personal fees from Roche, grants and personal fees from Merck, personal fees from AstraZeneca, personal fees from Bayer, personal fees and non-financial support from BMS, personal fees from Pharmamar, personal fees from Leo, outside the submitted work. The rest of the authors have nothing to disclose.
Figures

Similar articles
-
The epidemiology of oral human papillomavirus infection in healthy populations: A systematic review and meta-analysis.Oral Oncol. 2018 Jul;82:91-99. doi: 10.1016/j.oraloncology.2018.04.005. Epub 2018 May 21. Oral Oncol. 2018. PMID: 29909908
-
Human papillomavirus prevalence in oral and oropharyngeal squamous cell carcinoma in South America: A systematic review and meta-analysis.Oncol Rev. 2022 Mar 24;16(1):552. doi: 10.4081/oncol.2022.552. eCollection 2022 Feb 22. Oncol Rev. 2022. PMID: 35432780 Free PMC article.
-
Accuracy of Salivary Circulating Tumor Human Papillomavirus DNA in Detecting Oropharyngeal Cancer: A Systematic Review and Meta-Analysis.JAMA Otolaryngol Head Neck Surg. 2024 Jul 1;150(7):580-586. doi: 10.1001/jamaoto.2024.1067. JAMA Otolaryngol Head Neck Surg. 2024. PMID: 38780957 Free PMC article.
-
Systematic meta-analysis on association of human papilloma virus and oral cancer.J Cancer Res Ther. 2016 Apr-Jun;12(2):969-74. doi: 10.4103/0973-1482.179098. J Cancer Res Ther. 2016. PMID: 27461683
-
Human papillomavirus infections and upper aero-digestive tract cancers: the ARCAGE study.J Natl Cancer Inst. 2013 Apr 17;105(8):536-45. doi: 10.1093/jnci/djt053. Epub 2013 Mar 16. J Natl Cancer Inst. 2013. PMID: 23503618
Cited by
-
Human Papillomavirus 16 E6 Suppresses Transporter Associated with Antigen-Processing Complex in Human Tongue Keratinocyte Cells by Activating Lymphotoxin Pathway.Cancers (Basel). 2022 Apr 12;14(8):1944. doi: 10.3390/cancers14081944. Cancers (Basel). 2022. PMID: 35454851 Free PMC article.
-
miR-365 (microRNA): Potential Biomarker in Oral Squamous Cell Carcinoma Exosomes and Extracellular Vesicles.Int J Mol Sci. 2020 Jul 27;21(15):5317. doi: 10.3390/ijms21155317. Int J Mol Sci. 2020. PMID: 32727045 Free PMC article.
-
Papillomavirus Infection and Prevention: How Much Does the Sicilian Population Know? An Observational Study.Int J Environ Res Public Health. 2022 Sep 3;19(17):11032. doi: 10.3390/ijerph191711032. Int J Environ Res Public Health. 2022. PMID: 36078747 Free PMC article.
-
Salivary biomarkers: a promising approach for predicting immunotherapy response in head and neck cancers.Clin Transl Oncol. 2025 May;27(5):1887-1920. doi: 10.1007/s12094-024-03742-8. Epub 2024 Oct 8. Clin Transl Oncol. 2025. PMID: 39377974 Review.
-
Anal human papillomavirus infection among men who have sex with men and transgender women living with and without HIV in Pakistan: findings from a cross-sectional study.BMJ Open. 2021 Nov 1;11(11):e052176. doi: 10.1136/bmjopen-2021-052176. BMJ Open. 2021. PMID: 34725079 Free PMC article.
References
-
- Fakhry C., Westra W.H., Li S., Cmelak A., Ridge J.A., Pinto H., Forastiere A., Gillison M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008;100:261–269. doi: 10.1093/jnci/djn011. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
