

Comparison of breast cancer patients who underwent partial mastectomy (PM) with mini latissimus dorsi flap (MLDF) and subcutaneous mastectomy with implant (M + I) regarding quality of life (QOL), cosmetic outcome and survival rates
- PMID: 32370753
- PMCID: PMC7201547
- DOI: 10.1186/s12957-020-01858-z
Comparison of breast cancer patients who underwent partial mastectomy (PM) with mini latissimus dorsi flap (MLDF) and subcutaneous mastectomy with implant (M + I) regarding quality of life (QOL), cosmetic outcome and survival rates
Abstract
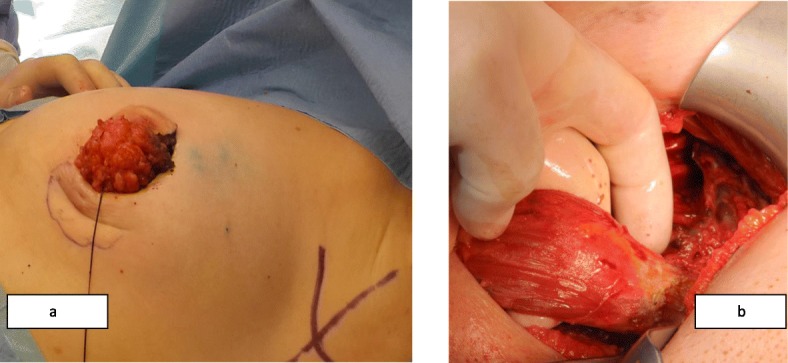
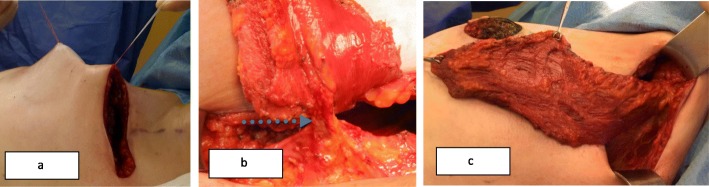
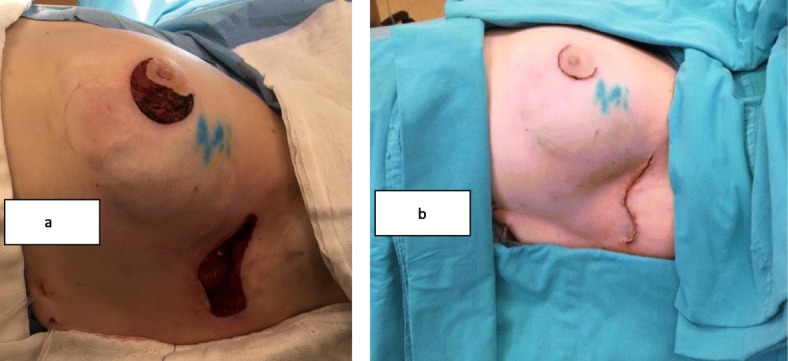
Purpose: The latissimus dorsi muscle has long been used in breast cancer (BC) patients for reconstruction. This study aimed to compare early stage BC patients who had partial mastectomy (PM) with mini latissimus dorsi flap (MLDF) and subcutaneous mastectomy with implant (MI) with respect to quality of life (QoL), cosmetic outcome (CO), and survival rates.
Patients and methods: The data of patients who underwent PM + MLDF (Group 1) and M + I (Group 2) between January 2010 and January 2018 were evaluated. Both groups were compared in terms of demographics, clinical and pathological characteristics, surgical morbidity, survival, quality of life, and cosmetic results. The EORTC-QLQ C30 and EORTC-QLO BR23 questionnaires and the Japanese Breast Cancer Society (JBCS) Cosmetic Evaluation Scale were used to assess the quality of life and the cosmetic outcome, respectively.
Results: A total of 317 patients were included in the study, 242 (76.3%) of them in group 1 and 75 (23.6%) of them in group 2. Median follow-up time was 56 (14-116) months. There were no differences identified between the groups in terms of tumor histology, hormonal receptors and HER-2 positivity, surgical morbidity, and 5-year overall and disease-free survival. Group 2 patients were significantly younger than group 1 (p = 0.003). The multifocality/multicentricity rate was higher in group 2 (p ≤ 0.001), whereas tumor size (p = 0.009), body mass index (BMI, p = 0.006), histological grade (p ≤ 0.001), lymph node positivity (p = 0.002), axillary lymph node dissection (ALND) rate (p = 0.005), and presence of lympho-vascular invasion (LVI, p = 0.013) were significantly higher in group 1. When the quality of life was assessed by using the EORTC QLQ C30 and BR23 questionnaires, it was seen that the body image perception (p < 0.001) and nausea/vomiting score (p = 0.024) were significantly better in PM + MLDF group whereas physical function score was significantly better in M + I group (p = 0.012). When both groups were examined in terms of cosmesis with JBCS Cosmetic Evaluation Scale, good cosmetic evaluation score was significantly higher in patients in MLDF group (p = 0.01).
Discussion: The results of this study indicate that in comparison to M + I procedure, the PM + MLDF procedure provides significantly superior results in terms of body image and cosmetic result with similar morbidity and oncologic outcomes. In selected patients with small breasts and a high tumor/breast ratio, PM + MLDF may be an alternative to subcutaneous mastectomy and implant.
Keywords: Breast-conserving surgery; Cosmetic evaluation; EORTC-QLO BR23; EORTC-QLO C30; Implant reconstruction; quality of life; Japanese breast cancer society cosmetic evaluation scale; Mini latissimus dorsi flap; Subcutaneous mastectomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018. 10.3322/caac.21492. - PubMed
-
- Bertozzi N, Pesce M, Santi PL, Raposio E. Oncoplastic breast surgery: comprehensive review. Eur Rev Med Pharmacol Sci. 2017;21(11):2572–2585. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
