

Electronic pillbox-enabled self-administered therapy versus standard directly observed therapy for tuberculosis medication adherence and treatment outcomes in Ethiopia (SELFTB): protocol for a multicenter randomized controlled trial
- PMID: 32370774
- PMCID: PMC7201596
- DOI: 10.1186/s13063-020-04324-z
Electronic pillbox-enabled self-administered therapy versus standard directly observed therapy for tuberculosis medication adherence and treatment outcomes in Ethiopia (SELFTB): protocol for a multicenter randomized controlled trial
Abstract
Background: To address the multifaceted challenges associated with tuberculosis (TB) in-person directly observed therapy (DOT), the World Health Organization recently recommended that countries maximize the use of digital adherence technologies. Sub-Saharan Africa needs to investigate the effectiveness of such technologies in local contexts and proactively contribute to global decisions around patient-centered TB care. This study aims to evaluate the effectiveness of pillbox-enabled self-administered therapy (SAT) compared to standard DOT on adherence to TB medication and treatment outcomes in Ethiopia. It also aims to assess the usability, acceptability, and cost-effectiveness of the intervention from the patient and provider perspectives.
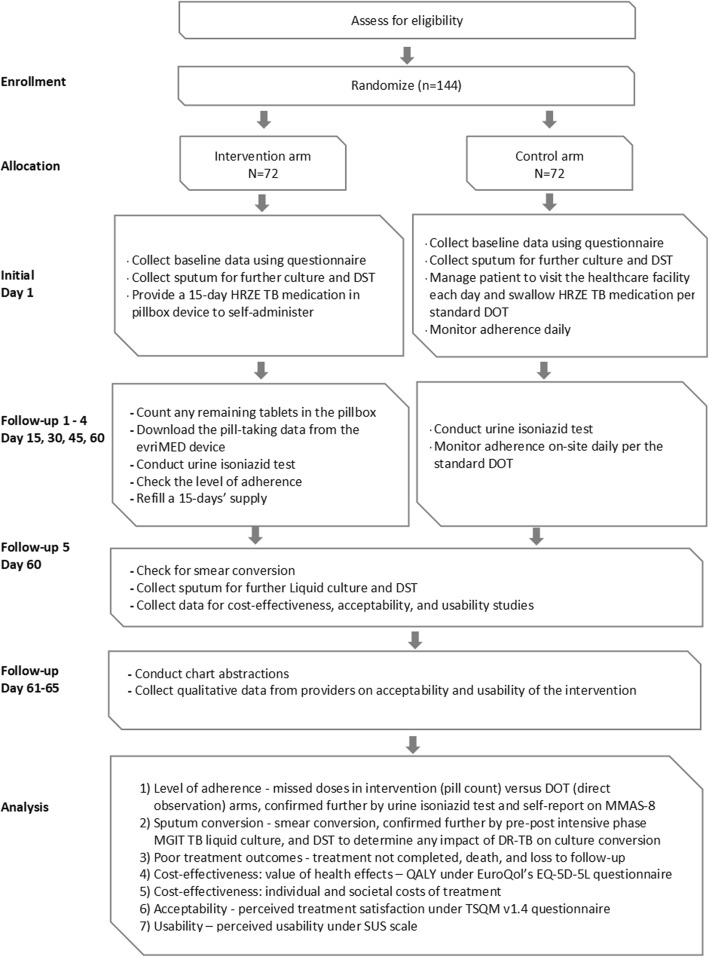
Methods: This is a multicenter, randomized, controlled, open-label, superiority, effectiveness-implementation hybrid, mixed-methods, two-arm trial. The study is designed to enroll 144 outpatients with new or previously treated, bacteriologically confirmed, drug-sensitive pulmonary TB who are eligible to start the standard 6-month first-line anti-TB regimen. Participants in the intervention arm (n = 72) will receive 15 days of HRZE-isoniazid, rifampicin, pyrazinamide, and ethambutol-fixed-dose combination therapy in the evriMED500 medication event reminder monitor device for self-administration. When returned, providers will count any remaining tablets in the device, download the pill-taking data, and refill based on preset criteria. Participants can consult the provider in cases of illness or adverse events outside of scheduled visits. Providers will handle participants in the control arm (n = 72) according to the standard in-person DOT. Both arms will be followed up throughout the 2-month intensive phase. The primary outcomes will be medication adherence and sputum conversion. Adherence to medication will be calculated as the proportion of patients who missed doses in the intervention (pill count) versus DOT (direct observation) arms, confirmed further by IsoScreen urine isoniazid test and a self-report of adherence on eight-item Morisky Medication Adherence Scale. Sputum conversion is defined as the proportion of patients with smear conversion following the intensive phase in intervention versus DOT arms, confirmed further by pre-post intensive phase BACTEC MGIT TB liquid culture. Pre-post treatment MGIT drug susceptibility testing will determine whether resistance to anti-TB drugs could have impacted culture conversion. Secondary outcomes will include other clinical outcomes (treatment not completed, death, or loss to follow-up), cost-effectiveness-individual and societal costs with quality-adjusted life years-and acceptability and usability of the intervention by patients and providers.
Discussion: This study will be the first in Ethiopia, and of the first three in sub-Saharan Africa, to determine whether electronic pillbox-enabled SAT improves adherence to TB medication and treatment outcomes, all without affecting the inherent dignity and economic wellbeing of patients with TB.
Trial registration: ClinicalTrials.gov, NCT04216420. Registered on 2 January 2020.
Keywords: Adherence; Directly observed therapy (DOT); Ethiopia; Pillbox; Self-administered therapy; Sub-Saharan Africa; Treatment outcome; Trials; Tuberculosis.
Conflict of interest statement
The authors declare that they have no competing interests.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
