

Impact of a preceding radiotherapy on the outcome of immune checkpoint inhibition in metastatic melanoma: a multicenter retrospective cohort study of the DeCOG
- PMID: 32371460
- PMCID: PMC7228559
- DOI: 10.1136/jitc-2019-000395
Impact of a preceding radiotherapy on the outcome of immune checkpoint inhibition in metastatic melanoma: a multicenter retrospective cohort study of the DeCOG
Abstract
Background: Immune checkpoint inhibition (ICI) is an essential treatment option in melanoma. Its outcome may be improved by a preceding radiation of metastases. This study aimed to investigate the impact of a preceding radiotherapy on the clinical outcome of ICI treatment.
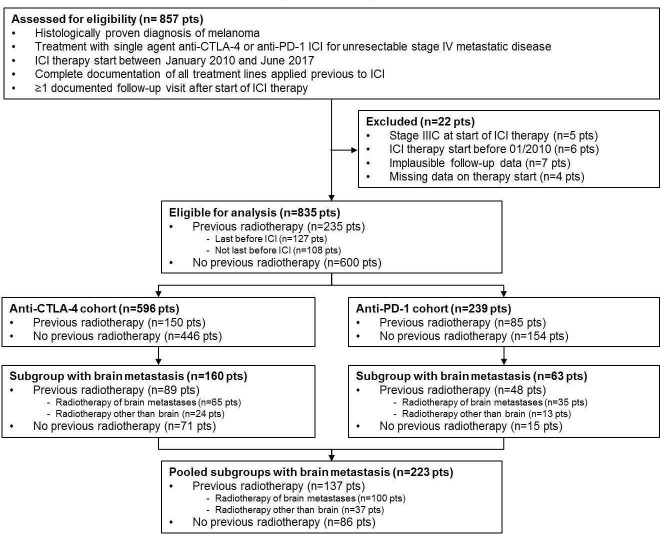
Methods: This multicenter retrospective cohort study included patients who received anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) or anti-programmed cell death protein 1 (PD-1) ICI with or without preceding radiotherapy for unresectable metastatic melanoma. ICI therapy outcome was measured as best overall response (BOR), progression-free (PFS) and overall survival (OS). Response and survival analyses were adjusted for confounders identified by directed acyclic graphs. Adjusted survival curves were calculated using inverse probability treatment weighting.
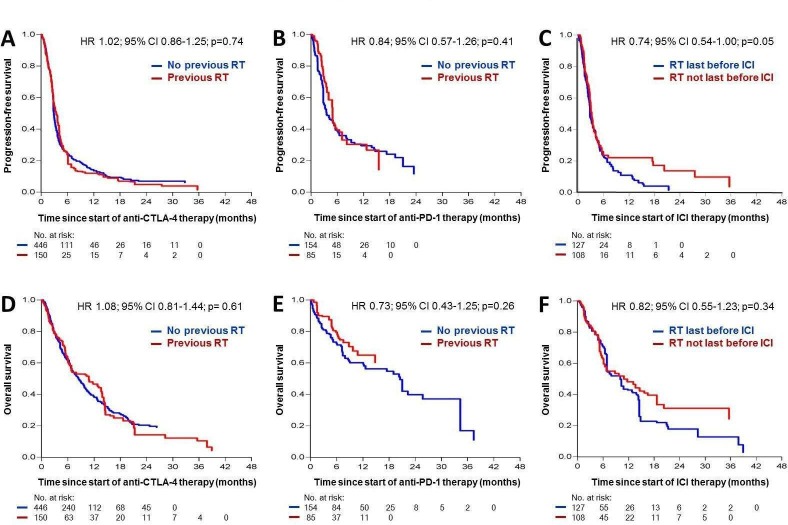
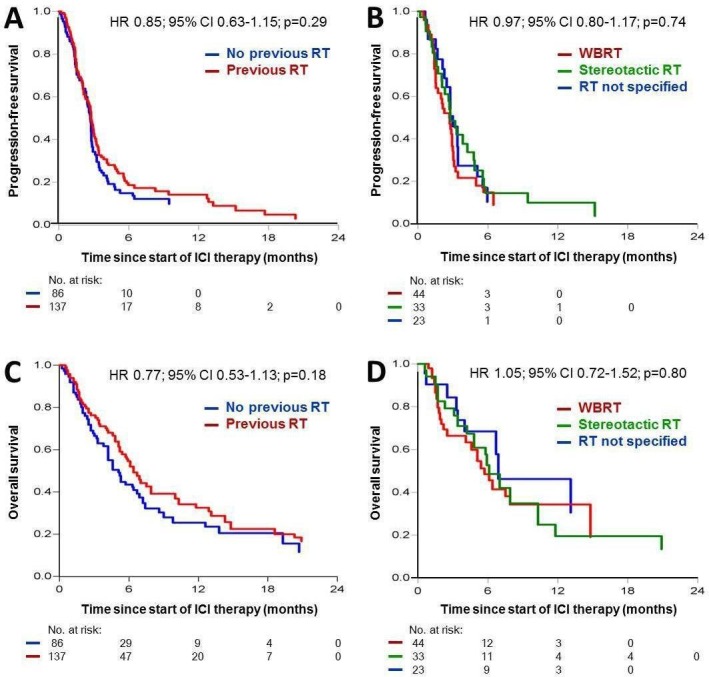
Results: 835 patients who received ICI (anti-CTLA-4, n=596; anti-PD-1, n=239) at 16 centers were analyzed, whereof 235 received a preceding radiotherapy of metastatic lesions in stage IV disease. The most frequent organ sites irradiated prior to ICI therapy were brain (51.1%), lymph nodes (17.9%) and bone (17.9%). After multivariable adjustment for confounders, no relevant differences in ICI therapy outcome were observed between cohorts with and without preceding radiotherapy. BOR was 8.7% vs 13.0% for anti-CTLA-4 (adjusted relative risk (RR)=1.47; 95% CI=0.81 to 2.65; p=0.20), and 16.5% vs 25.3% for anti-PD-1 (RR=0.93; 95% CI=0.49 to 1.77; p=0.82). Survival probabilities were similar for cohorts with and without preceding radiotherapy, for anti-CTLA-4 (PFS, adjusted HR=1.02, 95% CI=0.86 to 1.25, p=0.74; OS, HR=1.08, 95% CI=0.81 to 1.44, p=0.61) and for anti-PD-1 (PFS, HR=0.84, 95% CI=0.57 to 1.26, p=0.41; OS, HR=0.73, 95% CI=0.43 to 1.25, p=0.26). Patients who received radiation last before ICI (n=137) revealed no better survival than those who had one or more treatment lines between radiation and start of ICI (n=86). In 223 patients with brain metastases, we found no relevant survival differences on ICI with and without preceding radiotherapy.
Conclusions: This study detected no evidence for a relevant favorable impact of a preceding radiotherapy on anti-CTLA-4 or anti-PD-1 ICI treatment outcome in metastatic melanoma.
Keywords: immunology; oncology; radiotherapy.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SK has received travel support from Bristol-Myers Squibb and Amgen. AS received speaker honoraria from Merck Serono. LZ has served as consultant and/or has received honoraria from Roche, Bristol-Myers Squibb, Merck Sharp and Dohme, Novartis, Pierre Fabre, and Sanofi and has received travel support from Bristol-Myers Squibb, Merck Sharp and Dohme, Amgen, Pierre Fabre and Novartis. RG received honoraria for lectures and advisory boards, research support and meeting support from Almirall Hermal, Amgen, Astra Zeneca, Bristol-Myers Squibb, Leo, Merck Serono, Merck Sharp and Dohme, Pierre Fabre, Roche, Sanofi Genzyme, Regeneron, Sun Pharma, Takeda, Pfizer, Novartis, Johnson & Johnson, 4SC, and Incyte. LH has received grants from Novartis and has received personal fees from Amgen, Bristol-Myers Squibb, Merck Sharp and Dohme, Roche, Curevac, Pierre Fabre, Novartis and Sanofi. CW has served as consultant and/or has received honoraria from Amgen, Bristol-Myers Squibb, Curevac, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche, Sanofi, and Takeda, and has received travel support from Leo and Teva. CP received speaker or consultant honoraria and travel support from Novartis, Bristol-Myers Squibb, Roche, Merck Serono, Merck Sharp and Dohme, Celgene, AbbVie and LEO. AG reports speakers honoraria from Bristol-Myers Squibb, Merck Sharp and Dohme, and Roche; advisory board honoraria from Bristol-Myers Squibb, Novartis, Merck Sharp and Dohme, Pierre Fabre, Pfizer, Roche and Sanofi Genzyme; and travel support from Bristol-Myers Squibb, Merck Sharp and Dohme, Novartis, and Roche. RH declares speakers and advisory board honoraria from Bristol-Myers Squibb, Merck Sharp and Dohme, Novartis, and Roche. KCK has served as consultant and/or has received honoraria from Amgen, Roche, Bristol-Myers Squibb, Merck Sharp and Dohme, Pierre Fabre, and Novartis and has received travel support from Amgen, Merck Sharp and Dohme, Bristol-Myers Squibb, Amgen, Pierre Fabre, Medac, and Novartis. BW reports grants and personal fees from Bristol-Myers Squibb, Philogen and Merck Sharp and Dohme, and personal fees from Roche, Novartis, and Curevac. CB reports grants, personal fees, and non-financial support from Amgen, Bristol-Myers Squibb, Merck Sharp and Dohme, Merck Serono, Novartis, Roche, and 4SC, personal fees and non-financial support from Pierre Fabre and Sanofi Aventis as well as grants from Array Pharma and Regeneron. CL declares speakers and advisory board honoraria and travel support from Bristol-Myers Squibb, Merck Sharp and Dohme, Merck Serono, Novartis, Roche, Amgen, Pierre Fabre, and Sun Pharma. JU is on the advisory board or has received honoraria and travel support from Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Leo, Merck Sharp and Dohme, Novartis, Pierre Fabre, and Roche. PT has received speakers honoraria from Bristol-Myers Squibb, Novartis, Pierre Fabre and Roche, consultants honoraria from Bristol-Myers Squibb, Merck Serono, Novartis, Pierre Fabre and Roche, and travel support from Bristol-Myers Squibb and Pierre-Fabre. MK has received grants from Bristol-Myers Squibb, Merck Sharp and Dohme, Leo, Novartis and Roche. MS received honoraria for lectures from Merck Sharp and Dohme, Bristol-Myers Squibb, Roche, and Pierre Fabre, and served on advisory boards for Novartis, Roche, Merck Sharp and Dohme, and Pierre-Fabre. AK declares advisory board and speakers honoraria from Merck Sharp and Dohme, Sanofi Pasteur, and AbbVie. JU declares research support from Novartis, speakers and advisory board honoraria from Bristol-Myers Squibb, Merck Sharp and Dohme, Novartis, Roche and Sanofi, and travel support from Bristol Myers Squibb and Medac. PM declares research support from Bristol-Myers Squibb and Merck Sharp and Dohme, speakers and advisory board honoraria from Amgen, Bristol-Myers Squibb, Merck Sharp and Dohme, Merck Serono, Sanofi, Novartis, Roche, and Pierre Fabre, and travel support from Bristol-Myers Squibb, Merck Sharp and Dohme, Pierre Fabre and Novartis. EL has served as consultant or/and has received honoraria from Amgen, Actelion, Roche, Bristol-Myers Squibb, Merck Sharp and Dohme, Novartis, Janssen, Medac, and travel support from Amgen, Merck Sharp and Dohme, Bristol-Myers Squibb, Amgen, Pierre Fabre, and Novartis. JCB has received speakers honoraria from Amgen, MerckSerono, and Pfizer, advisory board honoraria from 4SC, Amgen, CureVac, eTheRNA, Lytix, MerckSerono, Novartis, Pfizer, Rigontec, and Sanofi as well as research funding from Alcedis, Bristol-Myers Squibb, Boehringer Ingelheim, IQVIA, and Merck Serono; he also received travel support from 4SC and Incyte. MW declares speakers and advisory board honoraria from Merck, Bristol-Myers Squibb, Roche, Novartis, Sanofi, Pierre Fabre, Beiersdorf, Sun Pharma, and Takeda. EC received travel support from Bristol-Myers Squibb, Merck Sharp and Dohme, and Novartis. DS declares advisory board and speakers honoraria from Roche, Novartis, Bristol-Myers Squibb, Merck, Amgen, Boehringer Ingelheim and Leo, as well as grant and travel support from Roche, Novartis, Bristol-Myers Squibb, Merck, Amgen, Boehringer Ingelheim and Leo. SU declares research support from Bristol-Myers Squibb and Merck Serono, speakers and advisory board honoraria from Bristol-Myers Squibb, Merck Sharp and Dohme, Merck Serono, Novartis, and Roche, and travel support from Bristol-Myers Squibb, Merck Sharp and Dohme. All remaining authors declared no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials