

Comparison of in-hospital and out-of-hospital cardiac arrest patients receiving targeted temperature management: A matched case-control study
- PMID: 32371666
- PMCID: PMC7478210
- DOI: 10.1097/JCMA.0000000000000343
Comparison of in-hospital and out-of-hospital cardiac arrest patients receiving targeted temperature management: A matched case-control study
Abstract
Background: Evidences that support the use of targeted temperature management (TTM) for in-hospital cardiac arrest (IHCA) are lacking. We aimed to investigate the hypothesis that TTM benefits for patients with IHCA are similar to those with out-of-hospital cardiac arrest (OHCA) and to determine the independent predictors of resuscitation outcomes in patients with cardiac arrest receiving subsequent TTM.
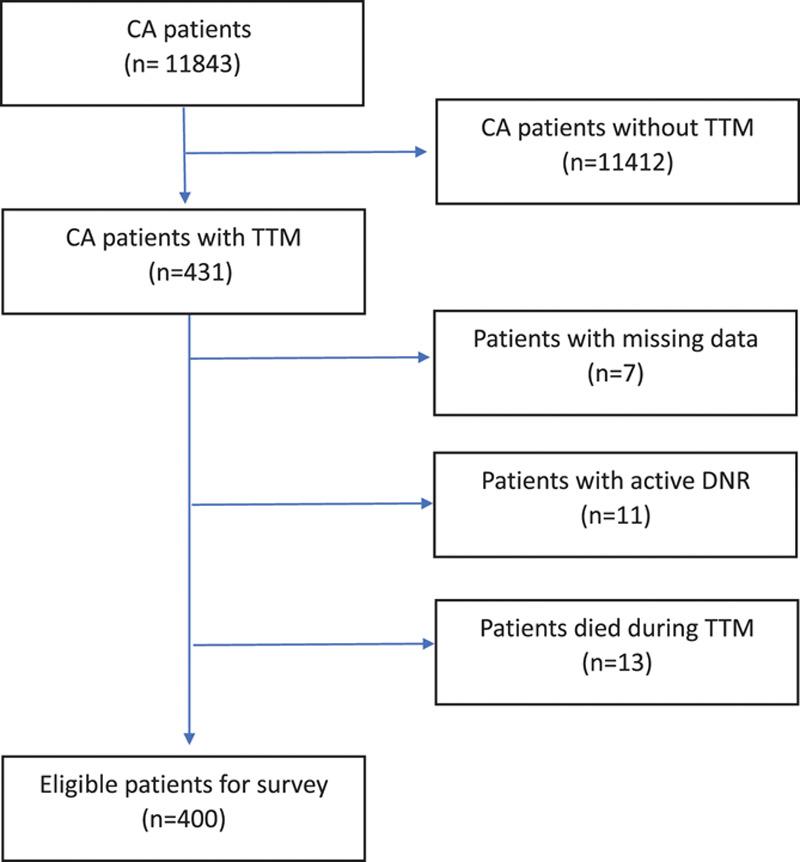
Methods: This is a retrospective, matched, case-control study (ratio 1:1) including 93 patients with IHCA treated with TTM after the return of spontaneous circulation, who were admitted to Partners HealthCare system in Boston from January 2011 to December 2018. Controls were defined as the same number of patients with OHCA, matched for age, Charlson score, and sex. Survival and neurological outcomes upon discharge were the primary outcome measures.
Results: Patients with IHCA were more likely to have experienced a witnessed arrest and receive bystander cardiopulmonary resuscitation, a larger total dosage of epinephrine, and extracorporeal membrane oxygenation. The time duration for ROSC was shorter in patients with IHCA than in those with OHCA. The IHCA group was more likely associated with mild thrombocytopenia during TTM than the OHCA group. Survival after discharge and favorable neurological outcomes did not differ between the two groups. Among all patients who had cardiac arrest treated with TTM, the initial shockable rhythm, time to ROSC, and medical history of heart failure were independent outcome predictors for survival to hospital discharge. The only factor to predict favorable neurological outcomes at discharge was initial shockable rhythm.
Conclusion: The beneficial effects of TTM in eligible patients with IHCA were similar with those with OHCA. Initial shockable rhythm was the only independent predictor of both survival and favorable neurological outcomes at discharge in all cardiac arrest survivors receiving TTM.
Conflict of interest statement
Conflicts of interest: The authors declare that they have no conflicts of interest related to the subject matter or materials discussed in this article.
Figures
Similar articles
-
Outcomes of Targeted Temperature Management for In-Hospital and Out-Of-Hospital Cardiac Arrest: A Matched Case-Control Study Using the National Database of Taiwan Network of Targeted Temperature Management for Cardiac Arrest (TIMECARD) Registry.Med Sci Monit. 2021 Jul 10;27:e931203. doi: 10.12659/MSM.931203. Med Sci Monit. 2021. PMID: 34244465 Free PMC article.
-
Similar long-term survival of consecutive in-hospital and out-of-hospital cardiac arrest patients treated with targeted temperature management.Clin Epidemiol. 2016 Nov 9;8:761-768. doi: 10.2147/CLEP.S114946. eCollection 2016. Clin Epidemiol. 2016. PMID: 27877067 Free PMC article.
-
In-hospital versus out-of-hospital cardiac arrest: Characteristics and outcomes in patients admitted to intensive care after return of spontaneous circulation.Resuscitation. 2022 Jul;176:1-8. doi: 10.1016/j.resuscitation.2022.04.023. Epub 2022 Apr 28. Resuscitation. 2022. PMID: 35490935
-
Survival to hospital discharge and neurological outcomes with targeted temperature management after in-hospital cardiac arrest: a systematic review and meta-analysis.Ann Palliat Med. 2022 Jan;11(1):68-76. doi: 10.21037/apm-21-3403. Ann Palliat Med. 2022. PMID: 35144399
-
Outcomes of Patients With in- and out-of-hospital Cardiac Arrest on Extracorporeal Cardiopulmonary Resuscitation: A Single-center Retrospective Cohort Study.Curr Probl Cardiol. 2023 May;48(5):101578. doi: 10.1016/j.cpcardiol.2022.101578. Epub 2022 Dec 30. Curr Probl Cardiol. 2023. PMID: 36587751 Review.
Cited by
-
Identifying Risk Factors for Prolonged Length of Stay in Hospital and Developing Prediction Models for Patients with Cardiac Arrest Receiving Targeted Temperature Management.Rev Cardiovasc Med. 2023 Feb 6;24(2):55. doi: 10.31083/j.rcm2402055. eCollection 2023 Feb. Rev Cardiovasc Med. 2023. PMID: 39077396 Free PMC article.
-
Effectiveness of Induced Hypothermia on the Prognosis of Post-cardiac Arrest Patients: A Scoping Literature Review.Cureus. 2023 Aug 7;15(8):e43064. doi: 10.7759/cureus.43064. eCollection 2023 Aug. Cureus. 2023. PMID: 37680442 Free PMC article.
-
Impact of cardiopulmonary resuscitation duration on functional outcome, level of independence, and survival among patients with in-hospital cardiac arrests: A pilot study.J Educ Health Promot. 2024 Aug 29;13:310. doi: 10.4103/jehp.jehp_1711_23. eCollection 2024. J Educ Health Promot. 2024. PMID: 39429822 Free PMC article.
-
Outcomes of Targeted Temperature Management for In-Hospital and Out-Of-Hospital Cardiac Arrest: A Matched Case-Control Study Using the National Database of Taiwan Network of Targeted Temperature Management for Cardiac Arrest (TIMECARD) Registry.Med Sci Monit. 2021 Jul 10;27:e931203. doi: 10.12659/MSM.931203. Med Sci Monit. 2021. PMID: 34244465 Free PMC article.
-
The association between C-reactive protein to albumin ratio and 6-month neurological outcome in patients with in-hospital cardiac arrest.World J Emerg Med. 2024;15(3):223-228. doi: 10.5847/wjem.j.1920-8642.2024.037. World J Emerg Med. 2024. PMID: 38855379 Free PMC article. No abstract available.
References
-
- Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008;118:2452–83. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002;346:557–63. - PubMed
-
- Hypothermia after Cardiac Arrest Study G Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346:549–56. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
