

Feasibility and accuracy of a robotic guidance system for navigated spine surgery in a hybrid operating room: a cadaver study
- PMID: 32371880
- PMCID: PMC7200720
- DOI: 10.1038/s41598-020-64462-x
Feasibility and accuracy of a robotic guidance system for navigated spine surgery in a hybrid operating room: a cadaver study
Abstract
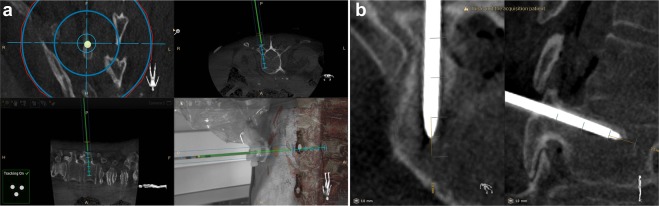
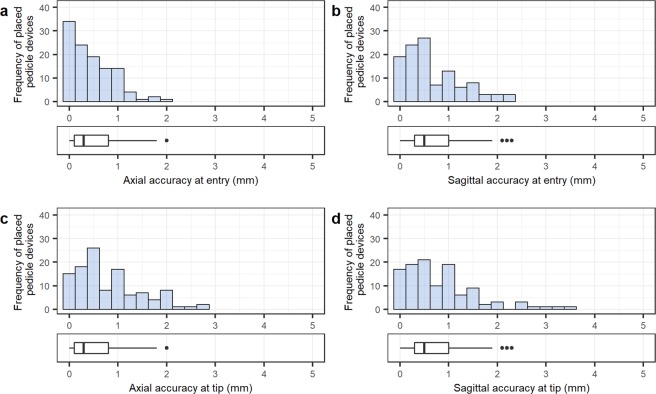
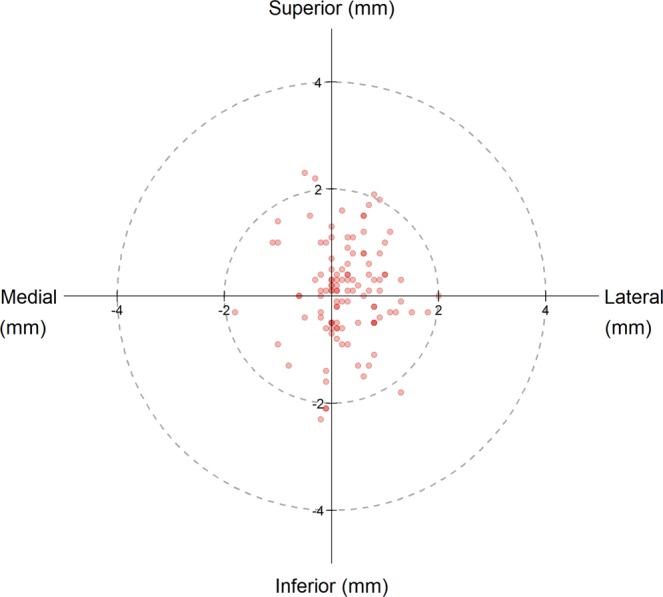
The combination of navigation and robotics in spine surgery has the potential to accurately identify and maintain bone entry position and planned trajectory. The goal of this study was to examine the feasibility, accuracy and efficacy of a new robot-guided system for semi-automated, minimally invasive, pedicle screw placement. A custom robotic arm was integrated into a hybrid operating room (OR) equipped with an augmented reality surgical navigation system (ARSN). The robot was mounted on the OR-table and used to assist in placing Jamshidi needles in 113 pedicles in four cadavers. The ARSN system was used for planning screw paths and directing the robot. The robot arm autonomously aligned with the planned screw trajectory, and the surgeon inserted the Jamshidi needle into the pedicle. Accuracy measurements were performed on verification cone beam computed tomographies with the planned paths superimposed. To provide a clinical grading according to the Gertzbein scale, pedicle screw diameters were simulated on the placed Jamshidi needles. A technical accuracy at bone entry point of 0.48 ± 0.44 mm and 0.68 ± 0.58 mm was achieved in the axial and sagittal views, respectively. The corresponding angular errors were 0.94 ± 0.83° and 0.87 ± 0.82°. The accuracy was statistically superior (p < 0.001) to ARSN without robotic assistance. Simulated pedicle screw grading resulted in a clinical accuracy of 100%. This study demonstrates that the use of a semi-automated surgical robot for pedicle screw placement provides an accuracy well above what is clinically acceptable.
Conflict of interest statement
M.B., A.Patriciu, S.K., A.Popovic, R. Holthuizen, and R. Homan are employed by Philips Research and/or Philips Healthcare. Karolinska University hospital and Philips Healthcare have a major collaboration agreement. All other authors have nothing to declare beyond the collaboration agreement of their employer. No author has a direct personal financial interest in the product.
Figures



Similar articles
-
Augmented and Virtual Reality Instrument Tracking for Minimally Invasive Spine Surgery: A Feasibility and Accuracy Study.Spine (Phila Pa 1976). 2019 Aug 1;44(15):1097-1104. doi: 10.1097/BRS.0000000000003006. Spine (Phila Pa 1976). 2019. PMID: 30830046
-
Pedicle screw accuracy in clinical utilization of minimally invasive navigated robot-assisted spine surgery.J Robot Surg. 2020 Jun;14(3):409-413. doi: 10.1007/s11701-019-00994-3. Epub 2019 Jul 19. J Robot Surg. 2020. PMID: 31321615 Free PMC article.
-
Decreasing the Pedicle Screw Misplacement Rate in the Thoracic Spine With Robot-guided Navigation.Clin Spine Surg. 2023 Dec 1;36(10):431-437. doi: 10.1097/BSD.0000000000001474. Epub 2023 Jun 16. Clin Spine Surg. 2023. PMID: 37348067 Free PMC article.
-
Safety and accuracy of robot-assisted placement of pedicle screws compared to conventional free-hand technique: a systematic review and meta-analysis.Spine J. 2021 Feb;21(2):181-192. doi: 10.1016/j.spinee.2020.09.007. Epub 2020 Sep 22. Spine J. 2021. PMID: 32976997
-
Robotic-assisted cortical bone trajectory (CBT) screws using the Mazor X Stealth Edition (MXSE) system: workflow and technical tips for safe and efficient use.J Robot Surg. 2021 Feb;15(1):13-23. doi: 10.1007/s11701-020-01147-7. Epub 2020 Sep 28. J Robot Surg. 2021. PMID: 32989623 Review.
Cited by
-
The Clinical Impact of Augmented Reality Surgical Navigation on Pedicle Screw Placement and its Effect on Perioperative Outcomes: A Systematic Review.Spine Surg Relat Res. 2024 Dec 10;9(3):269-282. doi: 10.22603/ssrr.2024-0223. eCollection 2025 May 27. Spine Surg Relat Res. 2024. PMID: 40503210 Free PMC article. Review.
-
Fluoroscopy-Guided Robotic System for Transforaminal Lumbar Epidural Injections.IEEE Trans Med Robot Bionics. 2022 Nov;4(4):901-909. doi: 10.1109/tmrb.2022.3196321. Epub 2022 Aug 4. IEEE Trans Med Robot Bionics. 2022. PMID: 37790985 Free PMC article.
-
Towards Optical Imaging for Spine Tracking without Markers in Navigated Spine Surgery.Sensors (Basel). 2020 Jun 29;20(13):3641. doi: 10.3390/s20133641. Sensors (Basel). 2020. PMID: 32610555 Free PMC article.
-
Navigation Techniques in Endoscopic Spine Surgery.Biomed Res Int. 2022 Aug 29;2022:8419739. doi: 10.1155/2022/8419739. eCollection 2022. Biomed Res Int. 2022. PMID: 36072476 Free PMC article. Review.
-
Augmented reality navigation in spine surgery: a systematic review.Acta Neurochir (Wien). 2021 Mar;163(3):843-852. doi: 10.1007/s00701-021-04708-3. Epub 2021 Jan 28. Acta Neurochir (Wien). 2021. PMID: 33506289 Free PMC article.
References
-
- Yoon JW, Wang MY. The evolution of minimally invasive spine surgery. J. Neurosurg. Spine. 2019;30:149–158. doi: 10.3171/2018.11.Spine181215. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
