

Clinical effectiveness of primary prevention implantable cardioverter-defibrillators: results of the EU-CERT-ICD controlled multicentre cohort study
- PMID: 32372094
- PMCID: PMC7550196
- DOI: 10.1093/eurheartj/ehaa226
Clinical effectiveness of primary prevention implantable cardioverter-defibrillators: results of the EU-CERT-ICD controlled multicentre cohort study
Abstract
Aims: The EUropean Comparative Effectiveness Research to Assess the Use of Primary ProphylacTic Implantable Cardioverter-Defibrillators (EU-CERT-ICD), a prospective investigator-initiated, controlled cohort study, was conducted in 44 centres and 15 European countries. It aimed to assess current clinical effectiveness of primary prevention ICD therapy.
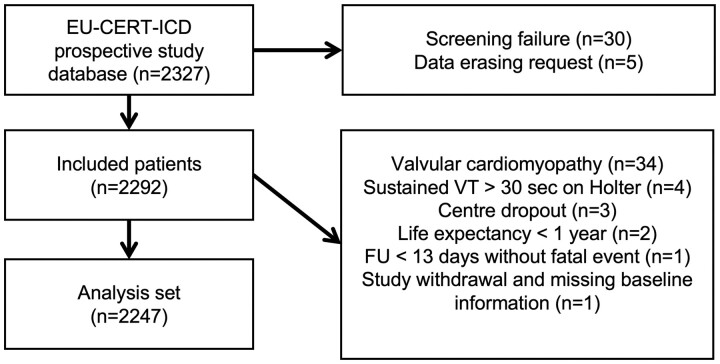
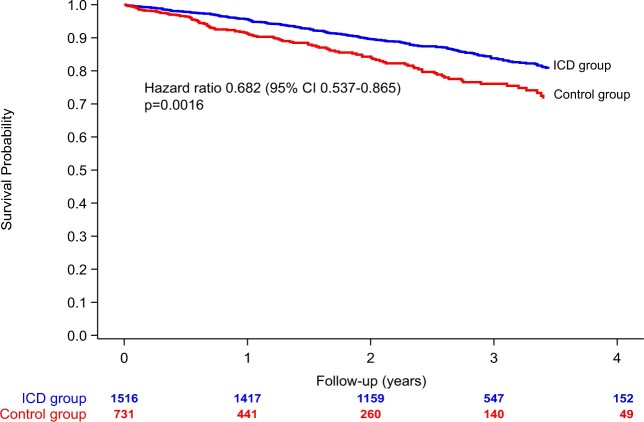
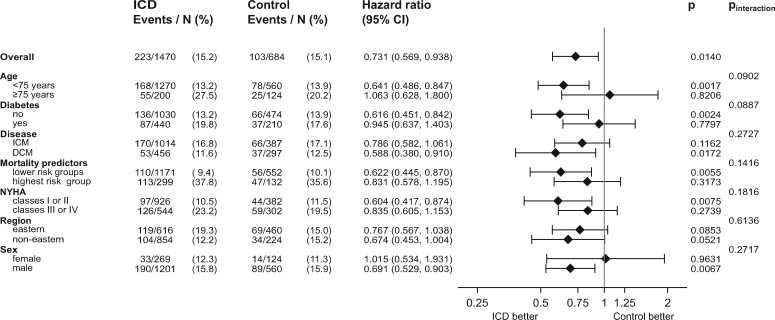
Methods and results: We recruited 2327 patients with ischaemic cardiomyopathy (ICM) or dilated cardiomyopathy (DCM) and guideline indications for prophylactic ICD implantation. Primary endpoint was all-cause mortality. Clinical characteristics, medications, resting, and 12-lead Holter electrocardiograms (ECGs) were documented at enrolment baseline. Baseline and follow-up (FU) data from 2247 patients were analysable, 1516 patients before first ICD implantation (ICD group) and 731 patients without ICD serving as controls. Multivariable models and propensity scoring for adjustment were used to compare the two groups for mortality. During mean FU of 2.4 ± 1.1 years, 342 deaths occurred (6.3%/years annualized mortality, 5.6%/years in the ICD group vs. 9.2%/years in controls), favouring ICD treatment [unadjusted hazard ratio (HR) 0.682, 95% confidence interval (CI) 0.537-0.865, P = 0.0016]. Multivariable mortality predictors included age, left ventricular ejection fraction (LVEF), New York Heart Association class <III, and chronic obstructive pulmonary disease. Adjusted mortality associated with ICD vs. control was 27% lower (HR 0.731, 95% CI 0.569-0.938, P = 0.0140). Subgroup analyses indicated no ICD benefit in diabetics (adjusted HR = 0.945, P = 0.7797, P for interaction = 0.0887) or those aged ≥75 years (adjusted HR 1.063, P = 0.8206, P for interaction = 0.0902).
Conclusion: In contemporary ICM/DCM patients (LVEF ≤35%, narrow QRS), primary prophylactic ICD treatment was associated with a 27% lower mortality after adjustment. There appear to be patients with less survival advantage, such as older patients or diabetics.
Keywords: Implantable cardioverter-defibrillator; Mortality; Risk factors; Sudden cardiac death.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Primary prevention of sudden death with the implantable cardioverter defibrillator: bridging the evidence gap.Eur Heart J. 2020 Sep 21;41(36):3448-3450. doi: 10.1093/eurheartj/ehaa324. Eur Heart J. 2020. PMID: 32424399 No abstract available.
-
Role of the proportion of sudden cardiac death to mortality for clinical effectiveness of primary prevention ICDs.Eur Heart J. 2020 Dec 14;41(47):4527-4528. doi: 10.1093/eurheartj/ehaa630. Eur Heart J. 2020. PMID: 32995841 No abstract available.
-
Is the clinical benefit of primary prevention implantable cardioverter-defibrillator overestimated? The role of sudden cardiac death to total mortality ratio.Eur Heart J. 2020 Dec 14;41(47):4525-4526. doi: 10.1093/eurheartj/ehaa580. Eur Heart J. 2020. PMID: 32995868 No abstract available.
References
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877–883. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005;352:225–237. - PubMed
-
- Kadish A, Dyer A, Daubert JP, Quigg R, Estes NA, Anderson KP, Calkins H, Hoch D, Goldberger J, Shalaby A, Sanders WE, Schaechter A, Levine JH; Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigator. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med 2004;350:2151–2158. - PubMed
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck K-H, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ; ESC Scientific Document Group. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. - PubMed
-
- Raatikainen MJ, Arnar DO, Merkely B, Camm AJ, Hindricks G. Access to and clinical use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology Countries: 2016 Report from the European Heart Rhythm Association. Europace 2016;18:iii1–iii79. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
