

Plasma pentraxin 3 is higher in early ovarian hyperstimulation syndrome than in uncomplicated in vitro fertilization cycle of high-risk women
- PMID: 32372340
- PMCID: PMC7246248
- DOI: 10.1007/s00404-020-05556-9
Plasma pentraxin 3 is higher in early ovarian hyperstimulation syndrome than in uncomplicated in vitro fertilization cycle of high-risk women
Abstract
Purpose: Pentraxin 3 (PTX3) is a locally secreted, quicker responsive pro-inflammatory protein than C-reactive protein (CRP). We evaluated the value of PTX3 in the prediction of ovarian hyperstimulation syndrome (OHSS), a severe complication of in vitro fertilization (IVF).
Methods: This two-year prospective follow-up study included 27 women with uncomplicated IVF-cycles (IVF group) and 31 patients diagnosed with moderate or severe early OHSS (OHSS group). PTX3 was analysed from follicular fluid (FF) and serial blood samples with enzyme-linked immunoassay and CRP with particle-enhanced immunoturbidimetric assay. The value of PTX3 and CRP in detecting OHSS was examined with receiver operating characteristic (ROC) curve analysis and expressed as the area under the curve (AUC).
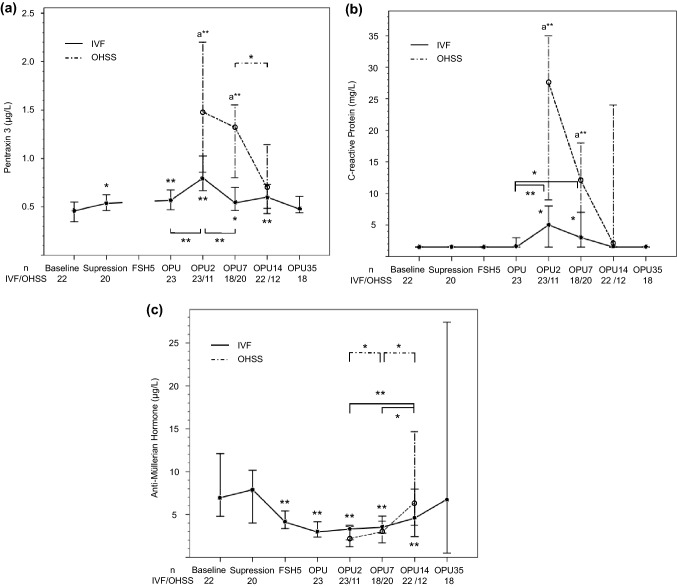
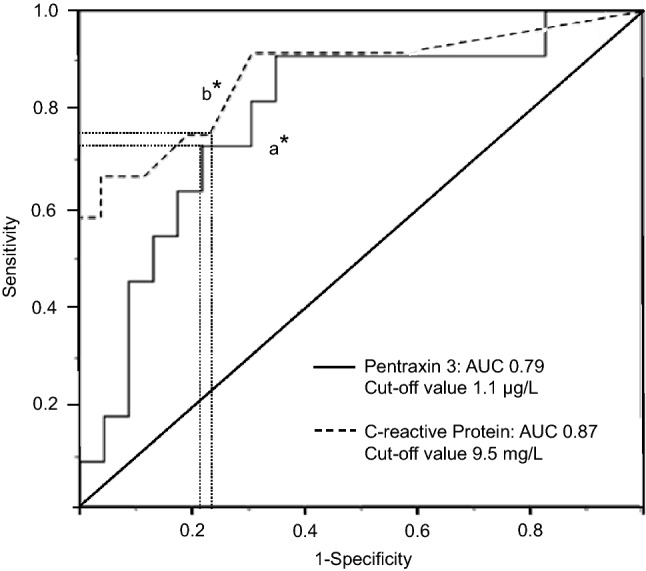
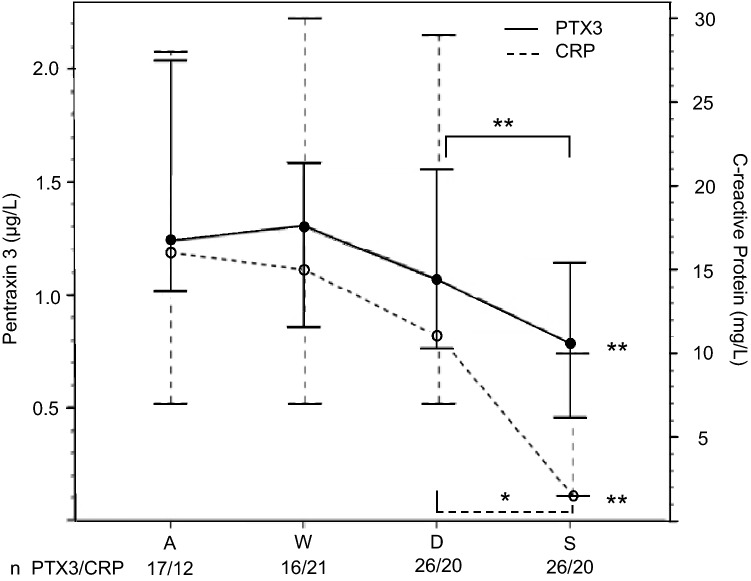
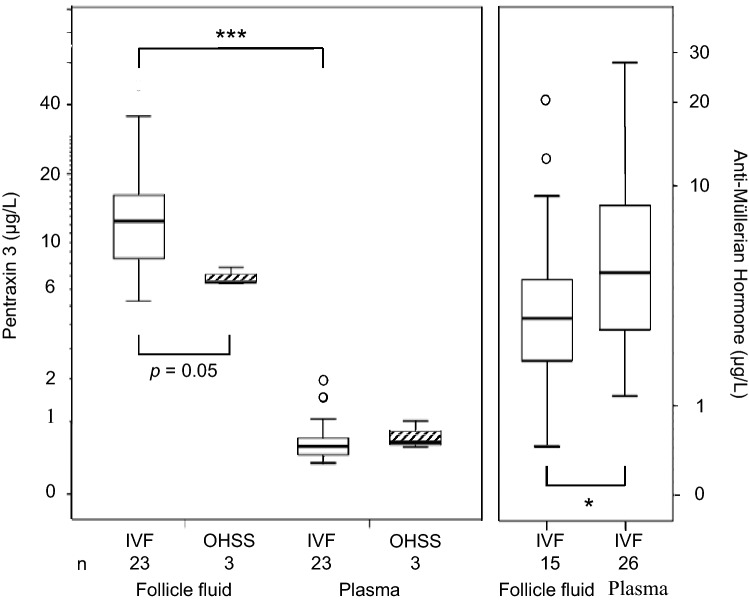
Results: The circulating PTX3 level peaked at two days after oocyte pick-up (OPU2), and in the OHSS group the level was 1.9 times higher (P = 0.006) than in the IVF group. However, in ROC curve analysis PTX3 (AUC 0.79, best cut off 1.1 µg/L) was not superior to CRP (AUC 0.87; best cut off 9.5 mg/L) in predicting early OHSS. In the IVF group, the FF-PTX3 concentration was 15-20 times higher than in the plasma. PTX3 level at OPU2 correlated with the number of punctured follicles (r = 0.56, n = 22, P = 0.006). Triggering with human chorionic gonadotrophin or early pregnancy had no effect on PTX3 level.
Conclusion: The elevated PTX3 concentration in OHSS at OPU2, when freeze-all embryos strategy is still possible to consider, indicates that PTX3 level could provide additional benefit in the risk assessment for early OHSS.
Conflict of interest statement
TM has received a speaker honorarium from Mylan and Astellas. HS-P has been a speaker for Mylan and received funding for congress trips from MSD. The other authors have no competing interests to declare.
Figures
Similar articles
-
C-reactive protein response is higher in early than in late ovarian hyperstimulation syndrome.Eur J Obstet Gynecol Reprod Biol. 2016 Dec;207:162-168. doi: 10.1016/j.ejogrb.2016.10.051. Epub 2016 Oct 31. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27865939
-
Risk of severe ovarian hyperstimulation syndrome in GnRH antagonist versus GnRH agonist protocol: RCT including 1050 first IVF/ICSI cycles.Hum Reprod. 2016 Jun;31(6):1253-64. doi: 10.1093/humrep/dew051. Epub 2016 Apr 8. Hum Reprod. 2016. PMID: 27060174 Clinical Trial.
-
Incidence and prediction of ovarian hyperstimulation syndrome in women undergoing gonadotropin-releasing hormone antagonist in vitro fertilization cycles.Fertil Steril. 2006 Jan;85(1):112-20. doi: 10.1016/j.fertnstert.2005.07.1292. Fertil Steril. 2006. PMID: 16412740 Clinical Trial.
-
Higher probability of live-birth in high, but not normal, responders after first frozen-embryo transfer in a freeze-only cycle strategy compared to fresh-embryo transfer: a meta-analysis.Hum Reprod. 2019 Mar 1;34(3):491-505. doi: 10.1093/humrep/dey388. Hum Reprod. 2019. PMID: 30689865
-
Ovarian hyperstimulation syndrome after superovulation using GnRH agonists for IVF and related procedures.Hum Reprod. 1992 Mar;7(3):320-7. doi: 10.1093/oxfordjournals.humrep.a137642. Hum Reprod. 1992. PMID: 1587936 Review.
Cited by
-
Vitamin D3 reduces the symptoms of ovarian hyperstimulation syndrome in mice and inhibits the release of granulosa cell angiogenic factor through pentraxin 3.In Vitro Cell Dev Biol Anim. 2024 Apr;60(4):432-440. doi: 10.1007/s11626-024-00898-z. Epub 2024 Apr 4. In Vitro Cell Dev Biol Anim. 2024. PMID: 38573397 Free PMC article.
-
PTX3/NF-κB/TLR4 Pathway Evaluation in the Follicular Fluid to Successfully Predict Blastocyst Implantation: A Pilot Study.Biomedicines. 2025 Apr 28;13(5):1071. doi: 10.3390/biomedicines13051071. Biomedicines. 2025. PMID: 40426899 Free PMC article.
-
Elevated plasma pentraxin-3 in polycystic ovary syndrome is associated with hyperandrogenism: a case-control study.BMC Endocr Disord. 2021 Dec 3;21(1):240. doi: 10.1186/s12902-021-00886-4. BMC Endocr Disord. 2021. PMID: 34856980 Free PMC article.
-
Serum erythropoietin level is increased during stimulation for IVF but not in OHSS.Reprod Biol Endocrinol. 2024 Jan 20;22(1):14. doi: 10.1186/s12958-023-01178-3. Reprod Biol Endocrinol. 2024. PMID: 38243286 Free PMC article.
References
-
- Herr D, Bekes I, Wulff C. Regulation of endothelial permeability in the primate corpora lutea: implications for ovarian hyperstimulation syndrome. Reproduction. 2015;149(2):R71–R79. - PubMed
-
- Wei LH, Chou CH, Chen MW, Rose-John S, Kuo ML, Chen SU, Yang YS. The role of IL-6 trans-signaling in vascular leakage: implications for ovarian hyperstimulation syndrome in a murine model. J Clin Endocrinol Metab. 2013;98(3):E472–E484. - PubMed
-
- Korhonen KVM, Savolainen-Peltonen HM, Mikkola TS, Tiitinen AE, Unkila-Kallio LS. C-reactive protein response is higher in early than in late ovarian hyperstimulation syndrome. EJOGRB. 2016;207:162–168. - PubMed
-
- Levin I, Gamzu R, Pauzner D, Rogowski O, Shapira I, Masloviz S, Almog B. Elevated levels of CRP in ovarian hyperstimulation syndrome: an unrecognised potential hazard? BJOG Int J Obstet Gynaecol. 2005;112(7):952–955. - PubMed
-
- Orvieto R, Chen R, Ashkenazi J, Ben-Harush A, Bar J, Fisch B. C-reactive protein levels in patients undergoing controlled ovarian hyperstimulation of IVF cycle. Hum Reprod. 2004;19(2):357–359. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
