

Small Animal Model of Post-chemotherapy Tuberculosis Relapse in the Setting of HIV Co-infection
- PMID: 32373548
- PMCID: PMC7176873
- DOI: 10.3389/fcimb.2020.00150
Small Animal Model of Post-chemotherapy Tuberculosis Relapse in the Setting of HIV Co-infection
Abstract
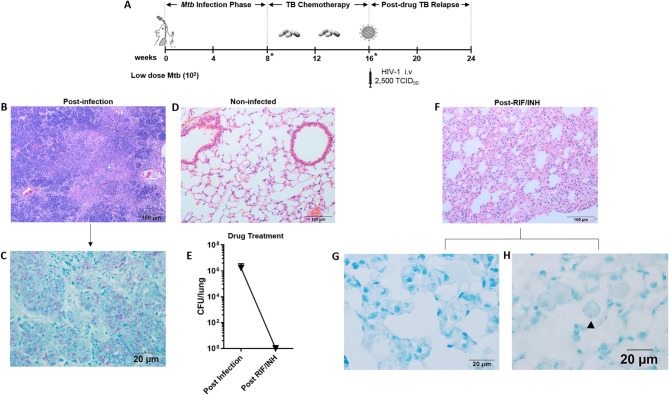
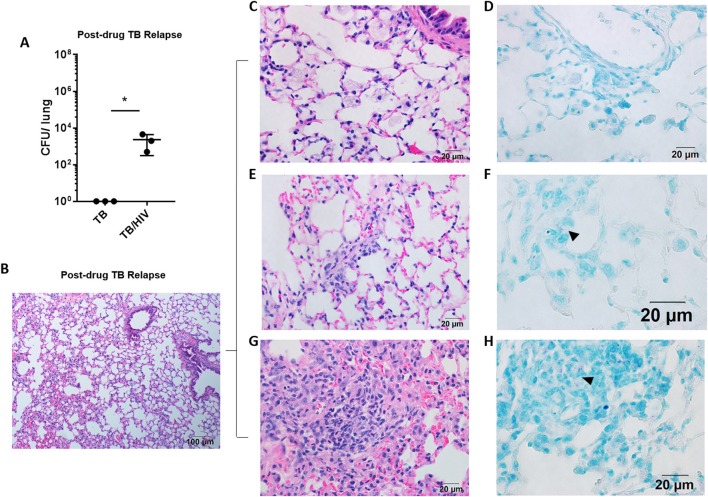
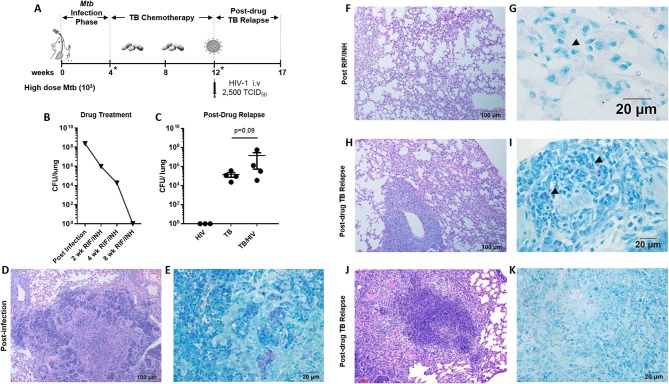
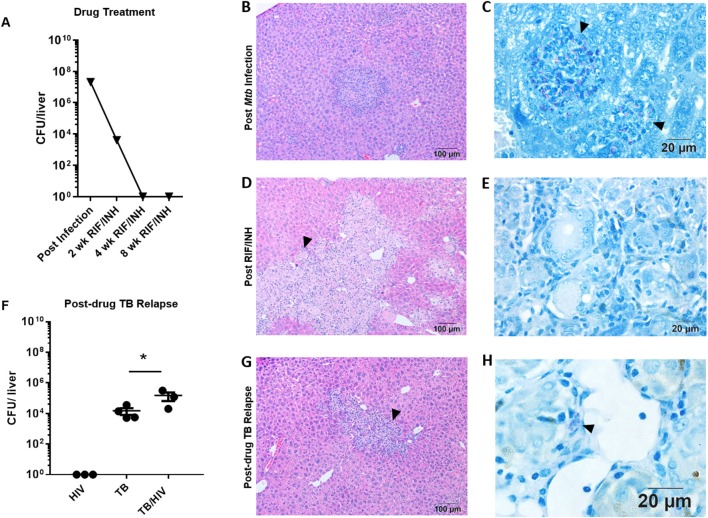
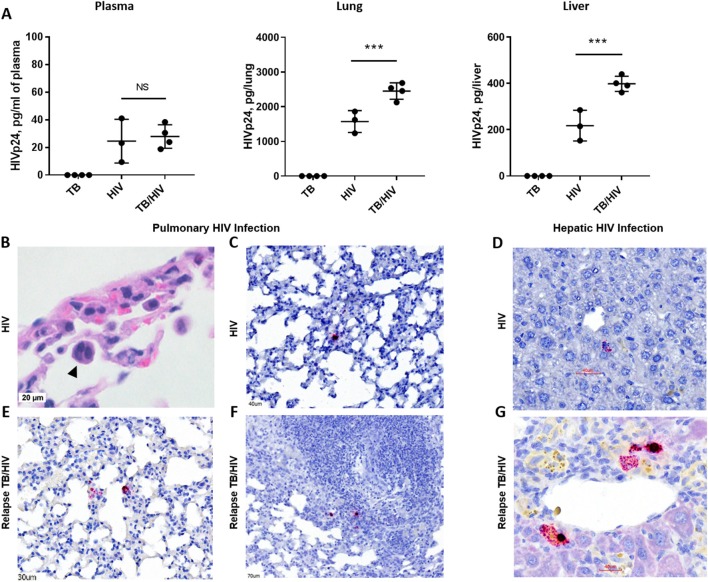
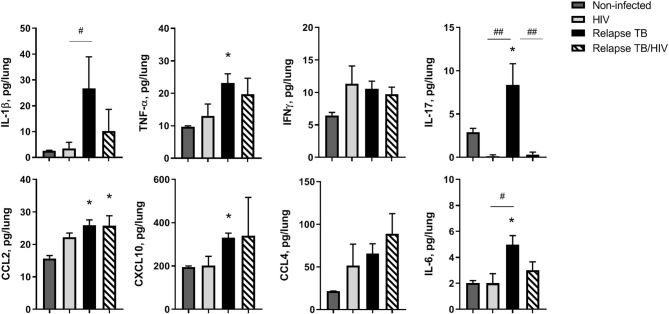
Tuberculosis relapse following drug treatment of active disease is an important global public health problem due to the poorer clinical outcomes and increased risk of drug resistance development. Concurrent infection with HIV, including in those receiving anti-retroviral therapy (ART), is an important risk factor for relapse and expansion of drug resistant Mycobacterium tuberculosis (Mtb) isolates. A greater understanding of the HIV-associated factors driving TB relapse is important for development of interventions that support immune containment and complement drug therapy. We employed the humanized mouse to develop a new model of post-chemotherapy TB relapse in the setting of HIV infection. Paucibacillary TB infection was observed following treatment with Rifampin and Isoniazid and subsequent infection with HIV-1 was associated with increased Mtb burden in the post-drug phase. Organized granulomas were observed during development of acute TB and appeared to resolve following TB drug therapy. At relapse, granulomatous pathology in the lung was infrequent and mycobacteria were most often observed in the interstitium and at sites of diffuse inflammation. Compared to animals with HIV mono-infection, higher viral replication was observed in the lung and liver, but not in the periphery, of animals with post-drug TB relapse. The results demonstrate a potential role for the humanized mouse as an experimental model of TB relapse in the setting of HIV. Long term, the model could facilitate discovery of disease mechanisms and development of clinical interventions.
Keywords: HIV; TB; TB and HIV co-infection; TB chemotherapy; TB relapse; immune response; pathology; tuberculosis.
Copyright © 2020 Huante, Saito, Nusbaum, Naqvi, Chauhan, Hunter, Actor, Rudra, Endsley, Lisinicchia, Gelman and Endsley.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical