

Comparison of Clinical Characteristics Between Febrile and Afebrile Seizures Associated With Acute Gastroenteritis in Childhood
- PMID: 32373562
- PMCID: PMC7176810
- DOI: 10.3389/fped.2020.00167
Comparison of Clinical Characteristics Between Febrile and Afebrile Seizures Associated With Acute Gastroenteritis in Childhood
Abstract
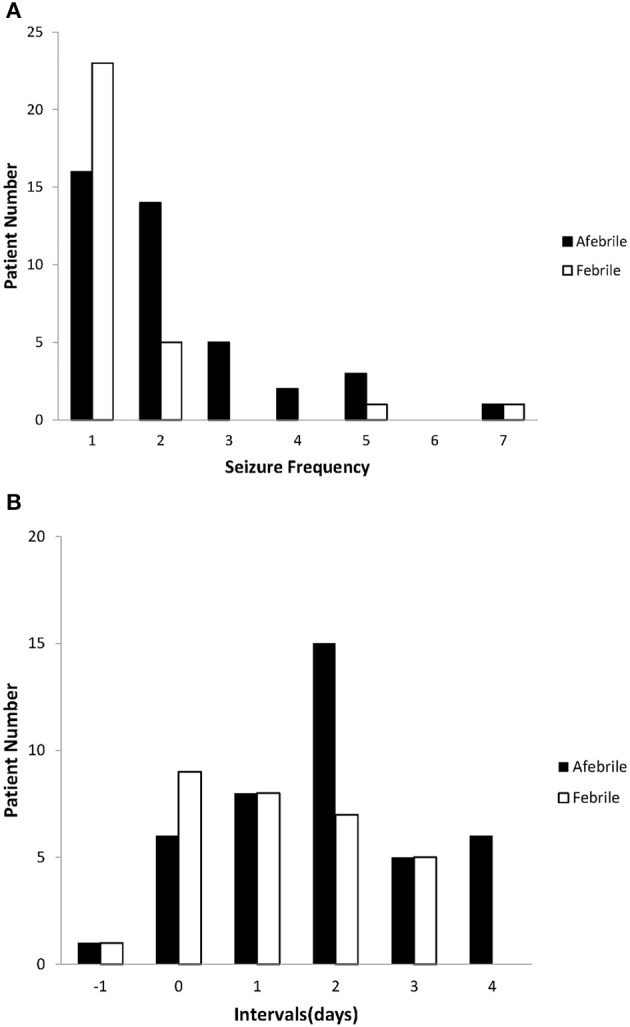
Background: Acute gastroenteritis (AGE) accompanied by seizures is not a rare scenario in childhood. We investigated the clinical features of children with febrile or afebrile seizures during AGE and aimed to identify the impact of fever in this situation-related seizure. Methods: We retrospectively reviewed the medical charts of children admitted due to seizures associated with mild AGE between January 2008 and December 2017. These consecutive patients were divided into two groups: an "afebrile group" whose diagnosis was compatible with "benign convulsion with mild gastroenteritis (CwG)" and a "febrile group" who had a fever within 24 h of the onset of an AGE-related seizure. We compared the two groups' clinical and laboratory characteristics, electroencephalograms (EEG), neuroimaging, and outcomes. Results: Of the children suffering from AGE and seizures, 41 were afebrile and 30 were febrile, with a mean age of 32.2 ± 27.6 months. The gender, seizure semiology, frequency, duration of seizures, the time interval between AGE symptoms onset and first seizure, and levels of serum sodium, and hepatic enzymes were significantly different between the two groups. The most frequently identified enteropathogen was rotavirus (33%), especially in the male and febrile subjects. Afebrile patients had more EEG abnormalities initially, but all returned to normal later. All cases had an uneventful outcome. Of note, seizure clusters (≥2 episodes) occurred more frequently in the afebrile patients who had a duration of AGE symptoms lasting 2 days or more, or white blood cell counts ≥ 10,000/μL (p-values: 0.05 and 0.04, respectively). In comparison with seven similar studies, all showed more seizure clusters, partial seizures, and a shorter interval between AGE onset and seizures in afebrile patients than in febrile patients. Contrarily, afebrile patients had longer seizure duration and lower serum hepatic transaminases than febrile patients. Conclusion: Although fever partially influenced the clinical features of AGE-related seizures, febrile CwG might have pathophysiology distinctly different from that of febrile seizures. Comprehensive knowledge in discerning febrile and afebrile CwG can help to avoid unnecessary diagnostics tests, and anticonvulsants use.
Keywords: acute gastroenteritis; afebrile; clinical features; comparison; fever; seizures.
Copyright © 2020 Wu, Liu, Tseng, Tseng and Chen.
Figures
Similar articles
-
Comparison between febrile and afebrile seizures associated with mild rotavirus gastroenteritis.Seizure. 2013 Sep;22(7):560-4. doi: 10.1016/j.seizure.2013.04.007. Epub 2013 May 1. Seizure. 2013. PMID: 23642407
-
A comparative study of febrile and afebrile seizures associated with mild gastroenteritis.Brain Dev. 2013 Aug;35(7):636-40. doi: 10.1016/j.braindev.2012.09.014. Epub 2012 Oct 27. Brain Dev. 2013. PMID: 23111347
-
Clinical characteristics of seizures associated with viral gastroenteritis in children.Epilepsy Res. 2015 Jan;109:146-54. doi: 10.1016/j.eplepsyres.2014.10.021. Epub 2014 Nov 6. Epilepsy Res. 2015. PMID: 25524854
-
Panayiotopoulos syndrome: a benign childhood autonomic epilepsy frequently imitating encephalitis, syncope, migraine, sleep disorder, or gastroenteritis.Pediatrics. 2006 Oct;118(4):e1237-43. doi: 10.1542/peds.2006-0623. Epub 2006 Sep 1. Pediatrics. 2006. PMID: 16950946 Review.
-
Benign afebrile convulsions in the course of mild acute gastroenteritis: a study of 28 patients and a literature review.Pediatr Emerg Care. 2011 Nov;27(11):1062-4. doi: 10.1097/PEC.0b013e31823b45b3. Pediatr Emerg Care. 2011. PMID: 22068069 Review.
Cited by
-
Febrile seizures and convulsions with mild gastroenteritis: age-dependent acute symptomatic seizures.Front Pediatr. 2023 Jul 18;11:1151770. doi: 10.3389/fped.2023.1151770. eCollection 2023. Front Pediatr. 2023. PMID: 37534200 Free PMC article. Review.
-
Update on benign convulsions with mild gastroenteritis.Clin Exp Pediatr. 2022 Oct;65(10):469-475. doi: 10.3345/cep.2021.00997. Epub 2021 Dec 27. Clin Exp Pediatr. 2022. PMID: 34961297 Free PMC article.
-
The baseline risk of multiple febrile seizures in the same febrile illness: a meta-analysis.Eur J Pediatr. 2022 Jun;181(6):2201-2213. doi: 10.1007/s00431-022-04431-w. Epub 2022 Mar 16. Eur J Pediatr. 2022. PMID: 35292852 Free PMC article.
-
Risk Factors for Benign Convulsions With Mild Gastroenteritis.Front Pediatr. 2022 Jun 29;10:925896. doi: 10.3389/fped.2022.925896. eCollection 2022. Front Pediatr. 2022. PMID: 35844760 Free PMC article.
-
Virus-Induced Epilepsy vs. Epilepsy Patients Acquiring Viral Infection: Unravelling the Complex Relationship for Precision Treatment.Int J Mol Sci. 2024 Mar 27;25(7):3730. doi: 10.3390/ijms25073730. Int J Mol Sci. 2024. PMID: 38612542 Free PMC article. Review.
References
-
- World Health Organization Causes of Child Mortality. (2017). Available online at: http://www.who.int/gho/child_health/mortality/causes/en (accessed 17 August, 2019).
-
- Morooka K. Convulsions and mild diarrhea. Shounika. (1982) 23:131–7.
LinkOut - more resources
Full Text Sources