

Posterior hypopyon in fungal endogenous endophthalmitis secondary to presumably contaminated dextrose infusion
- PMID: 32373756
- PMCID: PMC7191180
- DOI: 10.1016/j.ajoc.2020.100681
Posterior hypopyon in fungal endogenous endophthalmitis secondary to presumably contaminated dextrose infusion
Abstract
Purpose: To describe the presentation, clinical course and management of a patient with posterior hypopyon secondary to atypical (fungal) endogenous endophthalmitis.
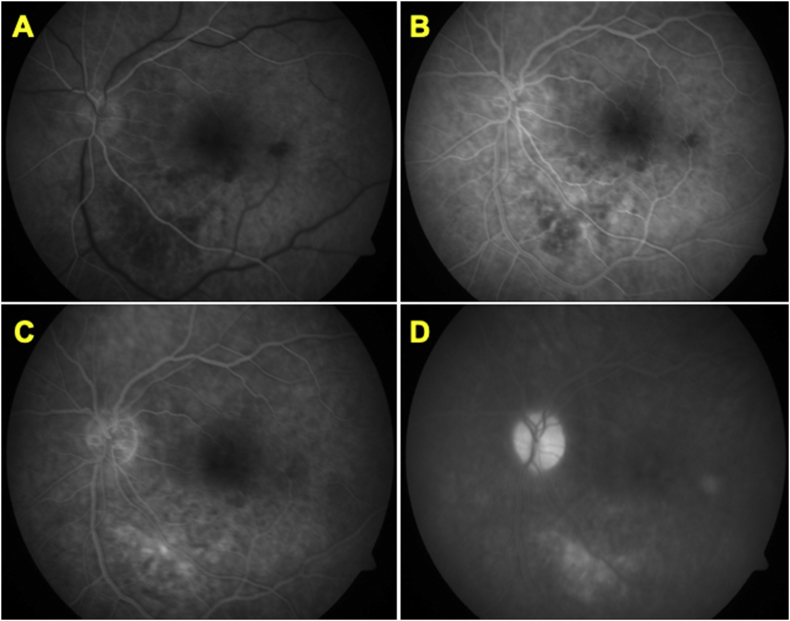
Observations: A 55-year-old Asian Indian female presented with decreased vision in the left eye (OS). The best-corrected visual acuity was 20/20 in the right eye (OD) and counting fingers (CF) in the left eye (OS) at the time of initial presentation. Slit-lamp examination revealed 1+ cells and 1+ flare in the anterior chamber of OS. Clinical examination and imaging assessment with fundus photography revealed vitritis, a posterior hypopyon and retinal exudates. The patient had an episode of fever one month before presentation for which an intravenous dextrose infusion was administered. After carefully evaluating the patient, ocular images, detailed history and necessary laboratory tests, a working diagnosis of endogenous endophthalmitis was reached. Empirical treatment with topical and systemic antibiotics, and topical cycloplegics and steroids was initiated. Therapeutic and diagnostic pars plana vitrectomy (PPV) was subsequently performed; microbiology and cytology analyses revealed evidence of fungal elements. Therefore, systemic anti-fungal treatment was initiated; the patient demonstrated significant clinical improvement with good visual outcome.
Conclusion and importance: Posterior hypopyon in endophthalmitis is a rarely observed entity and is typically obscured due to dense vitritis. Such clinical manifestation may suggest a possible infectious etiology as described in this case.
Keywords: Aspergillus; Contaminated infusions; Cytology; Dextrose; Endogenous endophthalmitis; Fungal; Immunocompetent; Posterior hypopyon.
© 2020 The Authors.
Conflict of interest statement
None for all authors.
Figures



References
-
- Romero C.F. Endogenous endophthalmitis: case report and brief review. Am Fam Physician. 1999;60(2):510–514. - PubMed
-
- Samiy N., D'Amico D.J. Endogenous fungal endophthalmitis. Int Ophthalmol Clin. 1996;36(3):147–162. - PubMed
-
- Simunovic M.P. Endophthalmitis following intravitreal injection versus endophthalmitis following cataract surgery: clinical features, causative organisms and post-treatment outcomes. Br J Ophthalmol. 2012;96(6):862–866. - PubMed
-
- Okada A.A. Endogenous bacterial endophthalmitis. Report of a ten-year retrospective study. Ophthalmology. 1994;101(5):832–838. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
